Abstract
Neurological symptoms and MRI changes post-sugammadex reversal
Liz Thaliath MD, Parker Chrisler BS, Deb Mojumder, MD, PhD
Corresponding author: Liz Thaliath
Contact Information: Thaliath.Liz@marshfieldclinic.org
DOI: 10.12746/swjm.v13i56.1493
ABSTRACT
Although sugammadex revolutionized anesthesia with rapid, effective reversal of non-depolarizing neuromuscular blocking agents, post-marketing surveillance identified rare occurrences of neurological side effects. To our knowledge, we report the first case of transient neurological symptoms and abnormal MRI changes following sugammadex administration. A 65-year-old woman underwent endoscopic resection of gastric lesion under general anesthesia. Sugammadex was used to reverse the non-depolarizing neuromuscular blocking agents. Preoperatively, she was alert with intact neurological function but postoperatively, she developed multiple neurological deficits. Magnetic resonance imaging (MRI) with diffusion-weighted imaging showed faint hyperintensity in the right temporal cortex. Despite an improved neurological exam, repeat diffusion-weighted imaging MRI revealed evolving hyperintensity in her bi-temporal cortex, and she returned to her baseline without residual deficits. A follow-up MRI on day 21 showed complete resolution. Notably, she had undergone a procedure five months earlier in which sugammadex had been used as a reversal agent and short-term neurological defects had been reported. Since other etiologies can cause some of these symptoms, we examined the specific and overall clinical context and argue against neuroinflammation or infectious etiology. Notably, neurological symptoms occurred following the only two occasions in which sugammadex was used to reverse rocuronium, while no adverse effects were reported when rocuronium was reversed using neostigmine in previous procedures. The mechanism of sugammadex causing transient neurological symptoms with MRI changes is unclear, but rat nerve cell culture studies indicate a possibility of neurotoxicity.
Keywords: Sugammadex, neuromuscular blocking agents, general anesthesia, neurotoxicity
INTRODUCTION
Sugammadex, introduced in Europe in 2008 and approved by the Federal Drug Administration in 2015, revolutionized anesthesia by providing rapid, effective reversal of non-depolarizing neuromuscular blocking agents (NMBAs) with minimal side effects. The key study that established its safety and efficacy for rocuronium reversal found that, while generally well-tolerated, mild and transient side effects like taste perversions and paresthesia also occurred. It also found that sugammadex facilitates faster post-anesthetic recovery compared to other traditionally used drugs like neostigmine.1
Sugammadex’s unique mechanism involves encapsulating NMBA molecules such as rocuronium and vecuronium via a cavity formed by its structure and Van der Waals forces. This 1:1 complex formation minimizes residual paralysis risk and allows for predictable dose-dependent reversal, enhancing safety and control.1–3 However, post-marketing surveillance and case reports have identified rare occurrences of early awakening, paradoxical prolonged blockades, and anaphylaxis.4 We present a unique case with focal neurological deficits and abnormal magnetic resonance imaging (MRI) brain findings suggestive of cortical involvement. The patient had a good recovery despite persistent abnormalities on MRI.
CASE
A 65-year-old Caucasian woman with a history of gastrointestinal stromal tumor and morbid obesity underwent partial endoscopic submucosal resection of a gastric lesion under general anesthesia. The anesthetic regimen included lidocaine (100 mg), propofol (160 mg), and rocuronium (70 mg). During the procedure, moderate bleeding occurred, and 10 cc of 1:10,000 epinephrine was administered. Her systolic blood pressure dropped from 180 mmHg to 80 mmHg, requiring phenylephrine (1300 mcg) to maintain a mean arterial pressure above 60 mmHg. Sugammadex (200 mg) was used to reverse the effects of rocuronium.
Preoperatively, the patient was alert, oriented, and had intact neurological function. Postoperatively, she presented with a rightward head turn, gaze deviation, incomprehensible speech, and an inability to follow commands. There was no withdrawal response to pain on the left side, and she had hemineglect affecting sensory and visual perception on the left side along with left-sided motor weakness. Differential diagnosis included acute ischemic and seizures. Delayed emergence from anesthesia seemed less likely due to focal neurological deficits. Computed tomography (CT) of the head ruled out intracranial hemorrhage, and CT angiography of the head and neck was negative for large vessel occlusion. Given her clinical presentation, Tenecteplase was administered. A challenge dose of midazolam (3 mg) did not change her neurological examination. Continuous electroencephalography revealed generalized slowing without seizure activity. Magnetic resonance imaging (Figure 1) with diffusion-weighted imaging (DWI) showed faint hyperintensity in the right temporal cortex. The apparent diffusion coefficient image showed corresponding signal changes, and fluid-attenuated inversion recovery (FLAIR) imaging revealed faint T2 hyperintensity in the corresponding region.
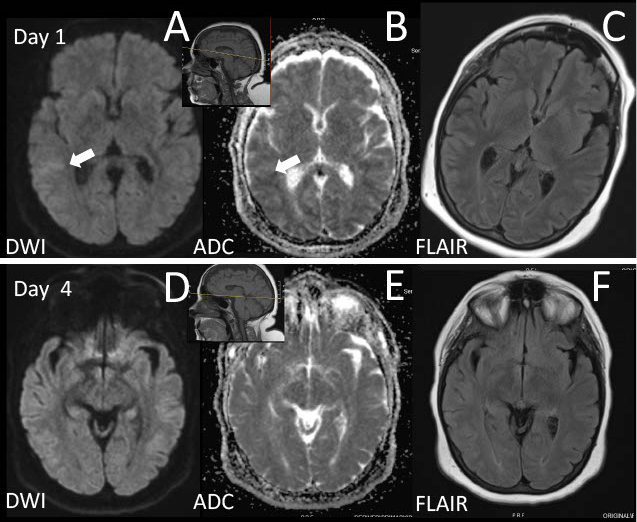
Figure 1. Top panel: MRI brain images on Day 1. A: Diffusion weighted image (DWI) showing faint hyperintensity in the right temporal cortex. B: ADC image showing signal changes corresponding A. C: FLAIR image showing faint T2 hyperintensity in the corresponding region. Top panel inset: Sagittal T1-weighted image showing reference line for top panel. Bottom Panel: MRI images on Day 4. D: Diffusion weighted image (DWI) now showing hyperintensity in bi-temporal cortex. E: ADC image showing minimal change. F: FLAIR images showing minimal change. Bottom panel inset: Sagittal T1-weighted image showing reference line for bottom panel.
By day 2, the patient showed significant neurological improvement. She could look to the left, answer simple questions, and follow commands. On day 3, her gaze was central, with mild left upper and lower extremity weakness and subtle left-sided visual neglect persisted.
By day 4, she had dramatically improved. Her neurological examination was non-focal, the left-sided visual neglect had resolved, and her speech impairment had significantly improved, with only mild word-finding difficulty. A repeat MRI (Figure 1) showed DWI hyperintensity in the bi-temporal cortex, with minimal changes on apparent diffusion coefficient and FLAIR images. By day 5, she returned to her baseline. A follow-up MRI (not shown) on day 21 indicated complete resolution of patchy DWI findings without residual FLAIR changes.
A review of the patient’s records revealed that five months prior, she underwent an esophagogastroduodenoscopy (EGD) and endoscopic ultrasound (EUS) under a general anesthetic regimen of lidocaine, propofol, rocuronium (25 mg), and sugammadex (200 mg). In this first instance of sugammadex use as an NMBA reversal agent in this patient, she exhibited a prolonged stuporous period, right-sided ocular drift, right-sided head tilt, and impaired speech, which resolved within four hours. Neurological symptoms occurred following the only two occasions in which sugammadex was used to reverse rocuronium. In contrast, no adverse effects were reported when rocuronium was reversed using neostigmine in previous surgical procedures in this patient (see Table 1).
Table 1. Demographic Characteristics of the Study Sample
Time
(Months/years prior to this episode) |
Procedure |
Anesthetic Regimen |
Outcome |
| 14 years |
Colonoscopy |
midazolam, fentanyl |
No side effects reported |
| 9 years |
Total abdominal hysterectomy with bilateral salpingo-oophorectomy |
fentanyl, ketamine, propofol, hydromorphone |
No side effects reported |
| 9 years |
EGD and Colonoscopy |
midazolam, fentanyl |
No side effects reported |
| 6 years |
EGD |
midazolam, fentanyl |
No side effects reported |
| 5 years |
radial EUS |
fentanyl, propofol, midazolam, lidocaine, succinylcholine |
no side effects reported |
| 4 years |
EGD and colonoscopy with polypectomy |
lidocaine, fentanyl, propofol, phenylephrine, rocuronium, neostigmine, glycopyrrolate |
no side effects reported |
| 5 months |
EGD with snare polypectomy and EUS |
lidocaine, propofol, rocuronium, sugammadex, glycopyrrolate |
neurological deficits observed (refer to case report) |
DISCUSSION
DWI and T2 alterations can be associated with various conditions, including hypoxia, ischemia, metabolic dysfunction, infections, seizures, neuroinflammation, and toxin exposure. The absence of documented hemodynamic instability or anoxic events during anesthesia suggests a low likelihood of global anoxia or significant perfusion deficits as the primary cause. Furthermore, the transient nature of the observed DWI changes and the subsequent reversal of neurological symptoms are atypical of anoxic brain injury, in which the deficits typically persist; initial DWI abnormalities evolve into pseudo-normalization around one week after the insult, followed by subsequent T2 changes.5 The areas of cortical restricted diffusion can also result from local vasospasm, especially considering the use of phenylephrine during anesthesia. However, such large areas would be expected from more proximal arterial vasospasm, which was not noted in the CT angiogram of this patient’s head and neck. Continuous electroencephalogram monitoring excluded seizure activity as a potential explanation for the DWI changes as well. The post-anesthetic presentation, rapid symptom resolution without immunomodulatory therapy, and the overall clinical context all argue against neuroinflammation or an infectious process as the underlying etiology.
The patent’s Naranjo score at was 6, suggesting a probable association between the adverse reaction and the administered drugs (sugammadex and rocuronium).6 Several other observations also support this conclusion. The adverse event manifested following the combined administration of sugammadex and rocuronium and resolved after a washout period, aligning with a potential causal link. Notably, similar reactions were not observed with past administrations of rocuronium alone. The patient’s history of similar reactions with the specific sugammadex and rocuronium combination further reinforces the likelihood of a drug-induced adverse event.
Sugammadex, a common reversal agent for neuromuscular blockade during surgery, has been linked to rare neurological side effects. These include anxiety, depression, dizziness, headaches, numbness, trouble sleeping, restlessness, muscle aches, and throat spasms.7 More rarely still, some patients regain consciousness right after receiving sugammadex, despite still being under anesthesia with other drugs.8 Studies suggest some potential mechanisms for these abnormal neurological presentations and MRI changes. Diffuse distal vasospasm of blood vessels in the brain might not be picked up by standard CTA imaging techniques, for instance.9 Sugammadex might have direct neurotoxic effects, as rat nerve cell cultures have shown sugammadex-triggered, mitochondria-dependent apoptosis in these cells, although sugammadex only has limited crossing of the blood-brain barrier.10 To the best of our knowledge, a similar combination of rocuronium and sugammadex causing neurological and MRI-brain changes has not been previously reported. This case highlights an avenue for future research.
ACKNOWLEDGEMENTS
The authors would like to thank David Puthoff, PhD at the Marshfield Clinic Research Center for their assistance with manuscript preparation.
REFERENCES
- Gijsenbergh F, Ramael S, Houwing N, et al. First human exposure of Org 25969, a novel agent to reverse the action of rocuronium bromide. Anesthesiology. 2005;103(4):695–703.
- Bom A, Bradley M, Cameron K, et al. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a cyclodextrin-based synthetic host. Angew Chem Int Ed Engl. 2002;41(2):266–70.
- Bom A, Hope F, Rutherford S, et al. Preclinical pharmacology of sugammadex. J Crit Care. 2009;24(1):29–35.
- Bridion solution for injection (sugammadex sodium) [product monograph]. Hertfordshire, UK; Merck Sharp & Dohme Limited; 2015.
- Mason Sharma A, Birnhak A, Sanborn E, et al. Neuroimaging mimics of anoxic brain injury: A review. Journal of Neuroimaging. 2023;33(4):467–76.
- Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–45.
- Bridion (sugammadex) injection [prescribing information]. Rahway, NJ: Merck Sharp & Dohme LLC; December 2024.
- Chazot T, Dumont G, Le Guen M, et al. Sugammadex administration results in arousal from intravenous anaesthesia: a clinical and electroencephalographic observation. British J Anaesthesia. 2011;106(6):914–16.
- Ko MJ, Kim YH, Kang E, et al. Cardiac arrest after sugammadex administration in a patient with variant angina: a case report. Korean J Anesthesiology. 2016;69(5):514.
- Palanca JM, Aguirre-Rueda D, Granell MV, et al. Sugammadex, a Neuromuscular Blockade Reversal Agent, Causes Neuronal Apoptosis in Primary Cultures. International J Med Sci. 2013;10(10):1278–85.
Article citation: Thaliath L, Chrisler P, Mojumder D. Neurological symptoms and MRI changes post-sugammadex reversal. The Southwest Journal of Medicine 2025;13(56):43–47
From: Department of Internal Medicine (LT), Marshfield Clinic; Wisconsin School of Medicine (PC); Department of Neurology (DM), Marshfield Clinic, Wisconsin, USA
Submitted: 3/27/2025
Accepted: 6/29/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.