Abstract
A rare case study: Adult orbital xanthogranulomatous disease
Megan Murchison MBA, MS, Addie Flowers MD, Meenu Sharma MD, Coby Ray MS, MD
Corresponding author: Coby Ray
Contact Information: Coby.Ray@ttuhsc.edu
DOI: 10.12746/swjm.v13i57.1501
ABSTRACT
This study contributes to the existing literature by exploring potential treatment options for the rare adult-onset subtype of orbital xanthogranulomatous disease, with the goal of improving diagnosis, management, and patient outcomes.
This case report presents a 28-year-old woman with bilateral periorbital swelling with prominent, firm yellow-orange lesions that had existed for over a year. These masses resulted in bilateral superior gaze restriction. Although high levels of rheumatoid factor were noted two months prior to surgery, all other biomarkers were within normal limits, which resulted in an inconclusive diagnosis until a biopsy of the mass was taken. The periorbital subcutaneous mass was treated surgically and excised successfully. Through histopathological examination, the presence of histiocytic infiltrate and multinucleated giant cells led to the diagnosis of adult orbital xanthogranulomatous disease (AOXD). Based on the histopathologic findings and absence of systemic involvement, the patient’s findings are consistent with adult-onset orbital xanthogranuloma (AOX) subtype. Adult-onset orbital xanthogranuloma is the rarest subtype of adult orbital xanthogranulomatous disease with varying treatment options, as there is no consensus on the most effective therapeutic course.
Keywords: Adult orbital xanthogranulomatous disease; histiocytes; multi-nucleated giant cells; histiocytic infiltrate
INTRODUCTION
Adult orbital xanthogranulomatous disease (AOXD) refers to a heterogeneous group of rare inflammatory diseases that are classified into 4 subtypes based on various clinical presentations: Adult-onset xanthogranuloma (AOX), necrobiotic xanthogranuloma, Erdheim-Chester disease, and adult-onset asthma and periocular xanthogranuloma.1 Each subtype features consistent histopathological findings of foamy histiocytes and multinucleated giant cells.1 This disease presents as bilateral diffuse or nodular lesions in the eyelid or orbit and can often be accompanied by systemic diseases such as hyperlipidemia, diabetes mellitus, or asthma.2 Patients can exhibit a range of symptoms, including displacement of the globe, restriction of the lid or eye movements, mechanical ptosis, diplopia, and decreased visual acuity.3,4 Orbital xanthogranuloma is often linked to hematological disorders, multiple myeloma, and non-Hodgkin lymphoma.3 However, with fewer than 50 reported cases in the literature, research on effective treatments is limited.5
CASE
A 28-year-old woman with no significant medical or ocular history was referred to the oculoplastics clinic for eyelid swelling. At presentation, the swelling had been present for over a year and was worsening. In addition to edema, her eyelids were pruritic and tender, and the patient occasionally rubbed her eyes due to the itching. The swelling affected her peripheral vision, and she felt her right eye was increasingly swollen, causing strain. She also noticed yellowing of her eyelids and more prominent veins (Figure 1).
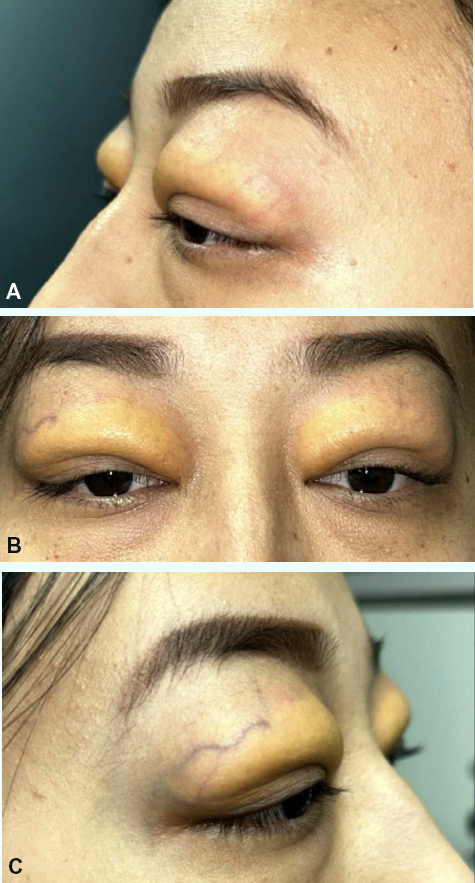
Figure 1. These images show the patient’s eyelids at the time of presentation to the oculoplastic clinic before surgery. This image shows the patient’s eyelids from the left profile (A), right profile (B), and front (C). These photos show bilateral subcutaneous orbital masses.
She had seen multiple doctors without a diagnosis or effective treatment for the edema. She had been treated for a stye, but the swelling persisted. During this time, she was hospitalized for COVID-19 and given a corticosteroid, which temporarily reduced the edema, but it returned afterward.
Her best corrected visual acuity was 20/30 OD and 20/25 OS. Her visual fields were full to confrontation bilaterally. There was upper lid edema present bilaterally with orange discoloration but no lagophthalmos. She had bilateral superior gaze restriction but otherwise normal ocular motility. Flipping her upper lids revealed a mild papillary reaction in both conjunctivae She was scheduled for a bilateral upper eyelid biopsy and debulking. (Should ‘bilaterally’ be before ‘papillary?’
Once in the OR, the patient’s eyelids were marked in the usual fashion for a blepharoplasty. A 15-blade was used to make the incision, and the eyelid skins were dissected superiorly. Just deep to the eyelid’s skin, a firm, rubbery, vascularized yellow mass was encountered. Samples were taken and sent to pathology. They were described as xanthogranulomatous inflammation with giant cells. The rest of the yellow mass was removed bilaterally, and more permanent sections were sent to pathology. The patient’s lids were closed with 6-0 proline beginning at the nasal aspect of the wound in a running fashion. After closure, it was noted that the patient had mild but symmetric lagophthalmos. Notably, on the day of surgery, the patient’s rheumatoid factor was 17 international units/mL (normal level 14 IU/mL). The patient had an unremarkable post-operative course. At four weeks postoperatively, she was doing well with no complaints.
Orbital MRI results at 8 months post-operatively showed bilateral lacrimal gland prolapse; however, no significant glandular edema (Figure 2). Extraocular muscles are symmetric, but more prominent than would be predicted for normal, particularly the lateral rectus muscle. There is mild enhancement within the pre-septal periorbital soft tissues.
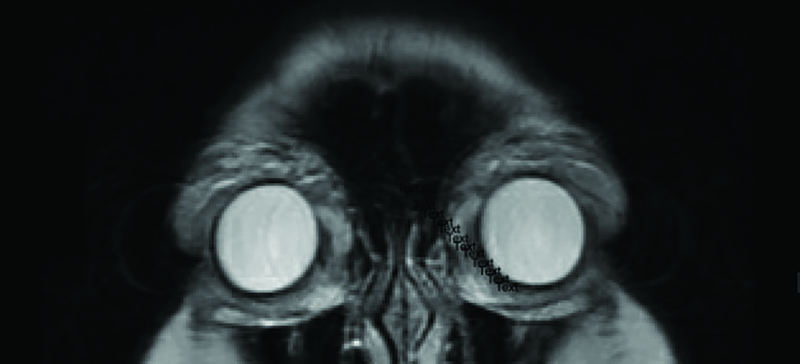
Figure 2. T2 anterior coronal MRI image 8 months post-operatively that demonstrates the density of the periorbital tissue of the upper and lower eyelids and lacrimal glands.
HISTOPATHOLOGY
Adult orbital xanthogranulomatous disease histopathological findings are consistent among the 4 sub-types.1 These findings are characterized by foamy histiocytes infiltrating the orbital tissue, with aggregates of lymphocytes, plasma cells, and Touton giant cells.1 Immunohistochemically, foamy histiocytes are strongly positive for CD68.1 In this case, orbital xanthogranulomatous disease has been diagnosed with histological support. Histopathology of the upper eyelid skin showed chronic inflammation with foamy histiocytes and Touton giant cells (Figure 3B). Imaging from the biopsy shows histiocytic infiltrate with mixed inflammatory cells and multinucleated giant cells (Figure 3A). Immunological staining is positive for cell marker CD68, which confirms the presence of foamy histiocytes (Figure 4). Based on these findings, the diagnosis of adult orbital xanthogranulomatous disease was confirmed.
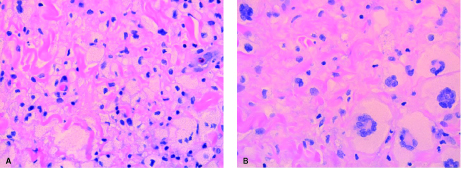
Figure 3. Hematoxylin and eosin stain: 40x showing histiocytic infiltrate with mixed inflammatory cells (A) and multinucleated giant cells (B).
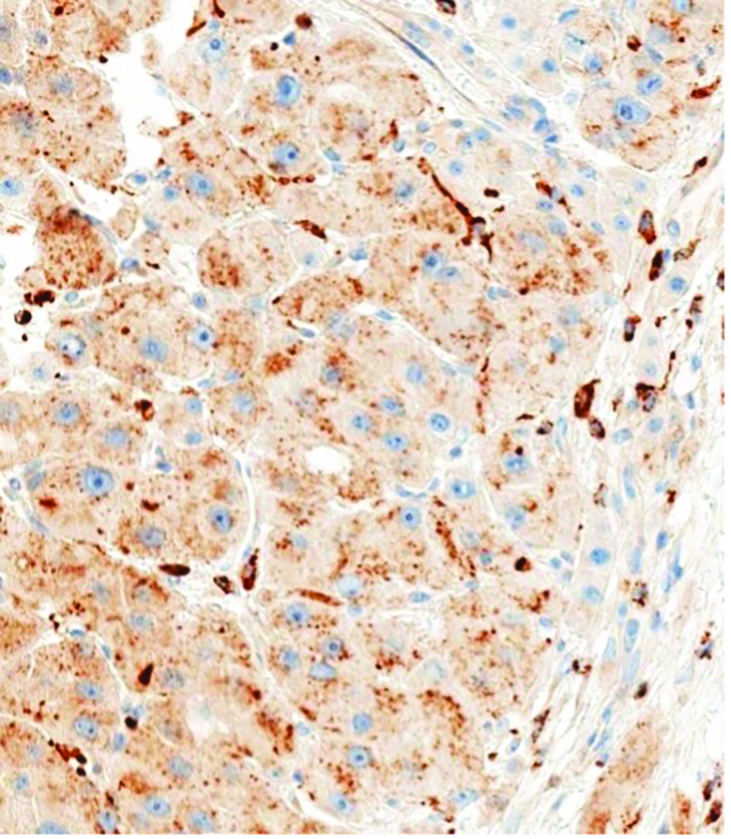
Figure 4. Immunological stain positive for cell-marker CD68.
DISCUSSION
Differentiating AOXD from xanthelasma palpebrarum is important. Xanthelasma, a cholesterol-rich eyelid deposition associated with lipid disorders, presents with foamy histiocytes but is confined to the dermis and contains esterified cholesterol in vacuoles, requiring clinicopathological correlation for diagnosis.8,9
Adult orbital xanthogranulomatous disease has four subtypes: Adult-onset (isolated lesions without systemic involvement), necrobiotic xanthogranuloma (associated with multiple myeloma and lymphomas), Erdheim-Chester disease (an idiopathic condition with systemic complications), and adult-onset asthma with periocular xanthogranuloma (features bilateral yellow/orange eyelid masses).1,6,7 Treatment depends on subtype and severity, with options such as surgery, corticosteroids, and chemotherapy showing varying success rates.10 Prognosis is good for adult-onset and asthma subtypes, while Erdheim-Chester and necrobiotic xanthogranuloma have poor outcomes.6
This patient presented with bilateral orange periorbital masses and a year-long history of eyelid swelling. Testing for autoimmune, endocrine, and infectious markers was negative, except for an elevated rheumatoid factor, suggesting an immunologically mediated mechanism. The lack of systemic symptoms pointed to the adult-onset subtype. Surgery improved visual acuity, though a small residual nasal mass remained on the right eye.
Adult orbital xanthogranulomatous disease, often linked to life-threatening conditions, has limited research on drug therapies and treatment options.2 The rare adult-onset subtype lacks data on its prevalence and outcomes, making diagnosis and treatment challenging. This leads to delays in treatment or misdiagnosis and ultimately affects the patient’s overall quality of life. Since AOXD involves an immunologically mediated process, further research could clarify underlying mechanisms and help develop new treatments. As therapies for autoimmune and inflammatory conditions evolve, their efficacy for AOXD could offer promising new management options. This study adds to the literature on potential surgical and therapeutic treatment options for the rare adult-onset subtype of orbital xanthogranulomatous disease.
PATIENT CONSENT
Written consent to publish this case has not been obtained. This report does not contain any personal identifying information.
ACKNOWLEDGMENTS AND DISCLOSURES
FUNDING SOURCES
No funding or grant support
CONFLICT OF INTEREST STATEMENT
The following authors have no financial disclosures: MM, AF, MS, CR.
AUTHORSHIP
All authors attest that they meet the current ICMJE criteria for Authorship.
ACKNOWLEDGMENTS
We would like to acknowledge the TTUHSC Department of Ophthalmology and its support of this work.
REFERENCES
- Guo J, Wang J. Adult orbital xanthogranulomatous disease: review of the literature. Arch Pathol Lab Med. 2009;133(12):1994–7.
- Shimizu F, Taneda H, Sato H, et al. A case of orbital xanthogranuloma treated by surgical excision. Case Rep Dermatol. 2010;2(2):110–15.
- Miszkiel KA, Sohaib SAA, Rose GE, et al. Radiological and clinicopathological features of orbital xanthogranuloma. Br J Ophthalmol. 2000;84(3):251–8.
- Wirth MA, Khan HM, Rasmussen SL, et al. Adult orbital xanthogranulomatous disease and myotonic dystrophy type 2: coexistence or association? Can J Ophthalmol. 2023;58(3):e136–e139.
- Green MB, Daly MK, Laver NMV, et al. Adult-onset asthma and periocular xanthogranuloma: a rare infiltrative disease of the orbit and eyelid. Am J Ophthalmol Case Rep. 2021;22:101043.
- Kerstetter J, Wang J. Adult orbital xanthogranulomatous disease: a review with emphasis on etiology, systemic associations, diagnostic tools, and treatment. Dermatol Clin.
- Davies MJ, Whitehead K, Quagliotto G, et al. Adult orbital and adnexal xanthogranulomatous disease. Asia Pac J Ophthalmol (Phila). 2017;6(5):435–43.
- Nair PA, Singhal R. Xanthelasma palpebrarum: a brief review. Clin Cosmet Investig Dermatol. 2017;11:1–5.
- Burris CK, Rodriguez ME, Raven ML, et al. Adult-onset asthma and periocular xanthogranulomas associated with systemic IgG4-related disease. Am J Ophthalmol Case Rep. 2016;1:34–7.
- Tekin B, Simsek IB, Akpinar R, et al. Adult orbital xanthogranulomatous disease: a case report and brief discussion of the terminology. Indian J Dermatol Venereol Leprol. 2016;82(5):547–50.
Article citation: Murchison M, Flower A, Sharma M, et al. A rare case study: Adult orbital xanthogranulomatous disease. The Southwest Journal of Medicine 2025;13(57):44–48
From: Texas Tech University Health Sciences Center School of Medicine, Lubbock, Texas (MM) Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas (AF) Department of Ophthalmology, Texas Tech University Health Sciences Center, Lubbock, Texas (CR) Department of Pathology, Texas Tech University Health Sciences Center, Lubbock, Texas (MS)
Submitted: 6/22/2025
Accepted: 9/15/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.