INTRODUCTION
Occupational interstitial lung diseases (ILDs) are a group of conditions resulting from exposure to dust, fumes, vapors, and biological agents.1 Considering the vast exposure, the prevalence of occupational ILDs is underappreciated. This is due to long latency periods, lack of standard diagnostic criteria, potential confounders, and non-standard surveillance practices.1 Occupational exposure causes various types of ILDs, including hypersensitivity pneumonitis, granulomatous diseases such as chronic beryllium disease or sarcoidosis, and pneumoconiosis.1–3 These can be differentiated from each other in terms of the latency period between exposure and diagnosis. A shorter latency period would indicate a current exposure, making hypersensitivity pneumonitis more probable, whereas a longer latency period would indicate pneumoconiosis.2
Due to the wide range of exposure eliciting lung injury in susceptible populations, we present an unusual case of occupational lung injury in a person who has made dental tools for the past twelve years. The uniqueness of the exposure and its association with lung disease without the presence of any confounding factors makes this a significant contribution to the understanding of occupational lung diseases. This case highlights the importance of identifying unique occupational exposures, such as dental tool fabrication, and their direct association with lung injury in the absence of other risk factors.
CASE
A 50-year-old man with no significant past medical history presented with complaints of shortness of breath and cough. He moved to the United States one year ago from Panama. He was admitted to the hospital with the complaint of severe dyspnea on exertion, associated with a non-productive cough, and concern that he was exposed to harmful chemicals at work, where he welded, soldered, and polished dental devices for the last twelve years. The patient used a hood but did not use a mask for protection. He reports no prior history of contact with pets and recent travel. He denied smoking and had not smoked in the past. His initial computed tomography (CT) scan showed diffuse reticulonodular opacities, mixed with patchy ground-glass opacities, more consolidative at the bases. The complete blood count and autoimmune workup were negative, and the echocardiogram was non-significant. He was treated with antibiotics for multifocal pneumonia and discharged in stable condition.
Despite the treatment, the shortness of breath continued to get worse, and he was not even able to walk 10 feet without stopping, which led to re-hospitalization a week later. Further workup was significant for positive T-Spot TB test, but the subsequent bronchoscopy and alveolar lavage (BAL) was non-significant and negative for active tuberculosis (TB). The high-resolution computed tomography (HRCT) [Figures 1–3] showed evidence of ongoing fibrosis, such as ground-glass opacities, subpleural sparing, reticulations, and traction bronchiectasis. The pulmonary function tests (PFTs) revealed forced vital capacity (FVC) of 1.54 L/40% predicted, forced expiratory volume in one second (FEV1) of 1.32 L/44% predicted, FEV1/FVC of 86% predicted [Table 1], and diffusing capacity for carbon monoxide (DLCO) of 24% predicted, concerning severe restrictive lung disease. He was treated with a four-drug regimen for TB and then rifampin for 2 more months, as the Quantiferon Gold Test was positive. Higher doses of prednisolone were also given multiple times for ILD. Wedge biopsies were obtained from each of the three lobes in the right lung, and they initially suggested usual interstitial pneumonitis (UIP). After seeking a second opinion from another facility, the diagnosis of nonspecific interstitial pneumonitis was also suggested. Each of the biopsies showed interstitial and intra-alveolar inflammatory processes with ongoing fibrosis, and foci of honeycombing and bronchiectasis. However, no definitive diagnosis could be established as hypersensitive features were also present but did not explain the constellation of findings. Due to the findings of NSIP and UIP, the plan was to start antifibrotics.

Figure 1. High-resolution computed tomography (HRCT). Red arrow: ground-glass opacities; blue arrow: subpleural reticulation.
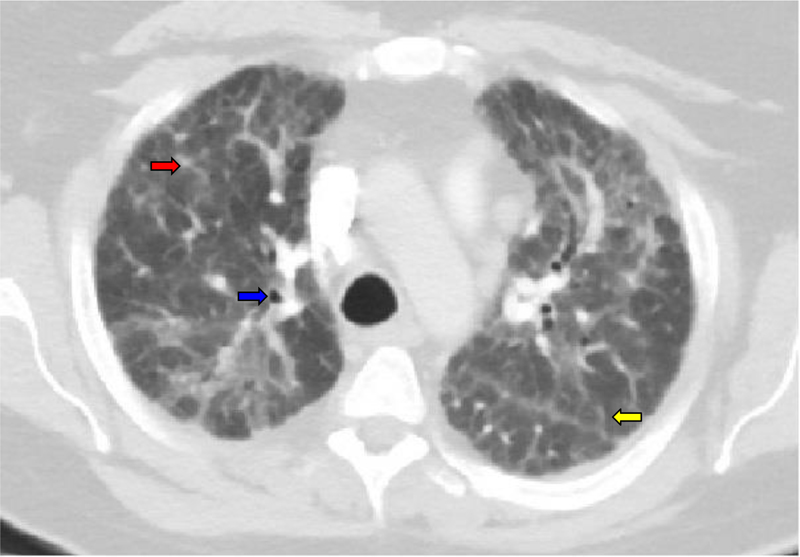
Figure 2. HRCT. Red arrow: ground-glass opacities; blue arrow: traction bronchiectasis, yellow arrow: reticulations.
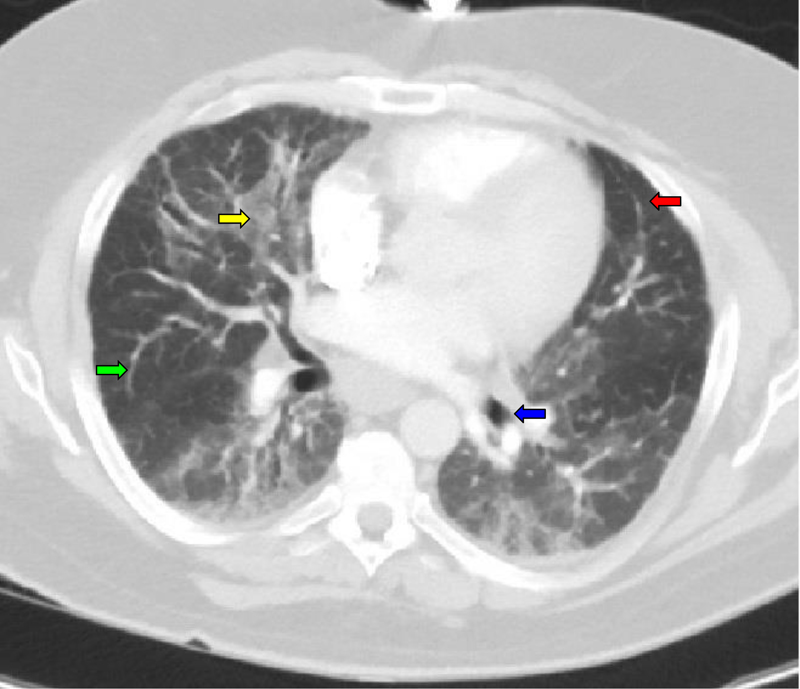
Figure 3. HRCT. Yellow arrow: ground-glass opacities; green arrow: reticulations; blue arrow: traction bronchiectasis; red arrow: subpleural sparing.
DISCUSSION
This patient’s occupation involved welding, soldering, and polishing dental devices, which indicated a possible link between occupational lung injury and this unusual exposure. The nature of his job made him susceptible to various exposures, including metal fumes, particulate matter, chemical vapors, gases, and allergic reactions to metals. The metals used in dental instruments are nickel, chromium, cadmium, lead, zinc, and beryllium. The absence of appropriate respiratory protection, as in this case, can cause occupational lung injury. The differential diagnoses included hypersensitivity pneumonitis (HP), pneumoconiosis, medication-induced pneumonitis, and idiopathic pulmonary fibrosis (IPF).
Hypersensitivity pneumonitis is a specific type of interstitial lung disease caused by an immune response to inhaled organic antigens, such as mold, bird droppings, or certain chemicals. The clinical findings are nonspecific, such as shortness of breath, cough, and expiratory crackles.4,5 Constitutional symptoms like fever and fatigue can also be present. Histologically, HP is characterized by lymphocytic infiltration of the lung interstitium and around small airways and non-necrotizing granulomas with collections of macrophages, sometimes surrounded by lymphocytes. This patient’s biopsy results confirmed the presence of interstitial and intra-alveolar inflammation. In another case report, microcalcification, non-caseating granuloma containing foreign body-type giant cells, and metal particles within macrophages in a dental technician were identified.4,6 However, the pathologists were not able to identify such metal particles in this patient. After chronic exposure to an eliciting substance, HP may progress to fibrosis and develop patterns that overlap with UIP or NSIP, exhibiting honeycombing, fibrotic scarring, and peribronchiolar fibrosis,4 some of which were present in this patient’s biopsy results. The absence of other HP features in this patient, like air trapping, centrilobular nodules, and upper/mid-sone predominance, was not conducive to the diagnosis of HP. Other lab results that may suggest HP include a lymphocyte count of >20%, although it was not present in this patient’s results.5
Chronic, progressive Interstitial fibrosis is also seen in IPF, which complicates the differentiation of HP from IPF. However, the IPF has a predominant UIP pattern on HRCT or lung biopsy, and it has no identifiable cause or exposure.7 Therefore, given the clear occupational history and radiologic and histologic features suggesting an inhalational antigen response, a diagnosis of IPF did not address current diagnostic criteria.
Pneumoconiosis was another consideration, as a case of pneumoconiosis has previously been identified in a dental technician.7 The imaging in pneumoconiosis had centrilobular nodules, and PFTs revealed a restrictive pattern. Subsequent analysis using energy-dispersive X-ray showed that the lung tissue contained metals such as indium, further confirmed by the elevated indium level. A cross-sectional study of 76 participants highlighted the prevalence of pneumoconiosis among dental technicians.8,9 Almost half of the participants had round opacities on HRCT and significantly reduced lung function in those with longer exposures. However, the HRCT in our patient lacked classic features such as upper-lobe predominant small nodules or progressive massive fibrosis, and wedge biopsy did not demonstrate dust-laden macrophages or retained inorganic particles. Elemental analysis or special stains could further rule this out definitively.
Medication-induced pneumonitis was another possibility in this patient, given his exposure to high-dose corticosteroids and anti-tuberculous treatment. Certain anti-tuberculosis drugs, such as rifampin and isoniazid, have been associated with drug-induced interstitial lung disease.10 It can also present with ground-glass opacities and a restrictive pattern on PFTs. However, in this patient, the initial symptoms began long before the start of anti-tubercular treatment. Furthermore, medication-induced pneumonitis typically improves with drug discontinuation and corticosteroid therapy. This further negated the possibility of medication-induced pneumonitis in this patient.
The overlapping features among HP, pneumoconiosis, and ILDs made diagnosing this patient challenging, but it drew attention toward this unique inhalation exposure. Although the multiple findings pointed to HP, others contradicted this diagnosis, preventing a definitive diagnosis. Given the progressive fibrosis, treatment with antifibrotic agents was an appropriate next step, with efforts to eliminate further occupational exposure.
CONCLUSION
This case presents a unique exposure of metal fumes from soldering and welding dental tools, causing interstitial lung disease. It can cause interstitial lung disease with overlapping features of HP, pneumoconiosis, and IPF. Although a definitive etiology could not be confirmed histologically in this patient, the clinical context of chronic occupational exposure to metal particles and the imaging findings suggested a likely exposure-related fibrosing ILD. Further research should focus on identifying the specific metal exposures associated with dental tool fabrication and their long-term respiratory effects, as well as developing appropriate preventative measures to protect workers in this industry.
REFERENCES
- Spagnolo P, Ryerson CJ, Guler S, et al. Occupational interstitial lung diseases. J Intern Med 2023 Dec;294(6):798–815. doi: 10.1111/joim.13707.
- Huntley CC, Moore CV. Occupational interstitial lung disease. Medicine, Volume 51, Issue 12:845–50.
- Reynolds C, Feary J, Cullinan P. Occupational contributions to interstitial lung disease. Clin Chest Med 2020 Dec;41(4):697–707. doi: 10.1016/j.ccm.2020.08.015.
- Costabel U, Miyazaki Y, Pardo A, et al. Hypersensitivity pneumonitis. Nat Rev Dis Primers 2020 Aug 6;6(1):65. doi: 10.1038/s41572-020-0191-z.
- Churg A. Hypersensitivity pneumonitis: new concepts and classifications. Mod Pathol 2022 Jan;35(Suppl 1):15–27. doi: 10.1038/s41379-021-00866-y.
- Kim YH, Chung YK, Kim C, et al. A case of hypersensitivity pneumonitis with giant cells in a female dental technician. Ann Occup Environ Med 2013 Oct 4;25(1):19. doi: 10.1186/2052-4374-25-19.
- Okamoto M, Tominaga M, Shimizu S, et al. Dental technicians’ pneumoconiosis. Intern Med 2017 Dec 15;56(24):3323–6. doi: 10.2169/internalmedicine.8860-17.
- Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med 2018;198(5):e44–e68. doi:10.1164/rccm.201807-1255ST
- Kahraman H, Koksal N, Cinkara M, et al. Pneumoconiosis in dental technicians: HRCT and pulmonary function findings. Occup Med (Lond) 2014 Sep;64(6):442–7. doi: 10.1093/occmed/kqu047.
- Skeoch S, Weatherley N, Swift AJ, et al. Drug-induced interstitial lung disease: a systematic review. J Clin Med 2018;7(10):356. doi:10.3390/jcm7100356
Article citation: Mazhar, IJ, Haider T, Khan A. Unique case of interstitial lung disease in a dental toolmaker. The Southwest Journal of Medicine 2025;13(56):48–52
From: Internal Medicine (IJM), Quaid-e-Azam Medical College, Pakistan; Hospital Medicine (TH), SSM Health St. Joseph St. Charles Hospital, Missouri; Pulmonary Medicine (AK), SSM Health St. Joseph St. Charles Hospital, Missouri
Submitted: 4/3/2025
Accepted: 7/1/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.