Abstract
A rare case of bronchopulmonary sequestration associated with a hiatal hernia
Abdul Hameed Zaid MBBS, Ali Abou-Yassine MD
Corresponding author: Abdul Hameed Zaid
Contact Information: Docahz@gmail.com
DOI: 10.12746/swjm.v13i57.1523
ABSTRACT
Bronchopulmonary sequestrations (BPS) are rare congenital anomalies resulting in formation of non-functioning lung tissue separate from the rest of the tracheobronchial tree. A defining feature of BPS is their arterial supply from an anomalous systemic vessel. Depending on pleural envelopment and venous drainage, they are categorized into intra-lobar (ILS) BPS and extra-lobar (ELS) BPS. In rare cases; they may be associated with other congenital pulmonary airway malformations and hiatal hernias. Bronchopulmonary sequestrations are usually identified on CT angiography and may be missed on non-contrast imaging. Definitive treatment typically involves embolization followed by surgical resection. We present a rare case of intra-lobar pulmonary sequestration associated with a hiatal hernia.
Keywords: bronchopulmonary sequestration, intra-lobar sequestration, hiatal hernia, congenital lung lesions, respiratory system abnormalities.
INTRODUCTION
First described in 1946 by Pryce,1 bronchopulmonary sequestrations (BPS) are rare congenital anomalies characterized by non-functioning lung tissue with no communication with the tracheobronchial tree.2 They are thought to originate during the pseudo-glandular stage of lung development before the separation of the aortic and pulmonary circulations3 and have anomalous systemic arterial blood supply. They are classified into two main types: Intra-lobar sequestrations (ILS), which are located within the visceral pleura of the adjacent normal lung with venous drainage into the pulmonary veins; and Extra-lobar sequestrations (ELS), which are enclosed in their own visceral pleura and typically drain into systemic veins, most commonly the inferior vena cava.4 In rare cases, sequestrations may be associated with congenital pulmonary airway malformations,5 bronchopulmonary foregut malformations6 and congenital diaphragmatic hernias.7 Asymptomatic sequestrations may be incidentally discovered on imaging but more commonly present as recurrent pneumonias.
CASE
A twenty-six-year-old man with a history of ulcerative colitis presented to our emergency room with severe epigastric pain and vomiting. Computed tomography (CT) of abdomen showed a gastric volvulus associated with a large incarcerated hiatal hernia (Figure 1). The patient underwent gastric decompression followed by urgent diagnostic laparoscopy, reduction and repair of the hernia, and fundoplication. The patient was discharged from the hospital the following day but returned two weeks later with shortness of breath and chest tightness. A CT angiogram revealed a left lung pneumonia and a loculated pleural effusion. Empiric antimicrobials were initiated to treat pneumonia and empyema. A closer review of imaging revealed that part of the left lung base was receiving direct blood supply from the aorta and a branch of the celiac trunk leading to the identification of an infected BPS (Figure 2).
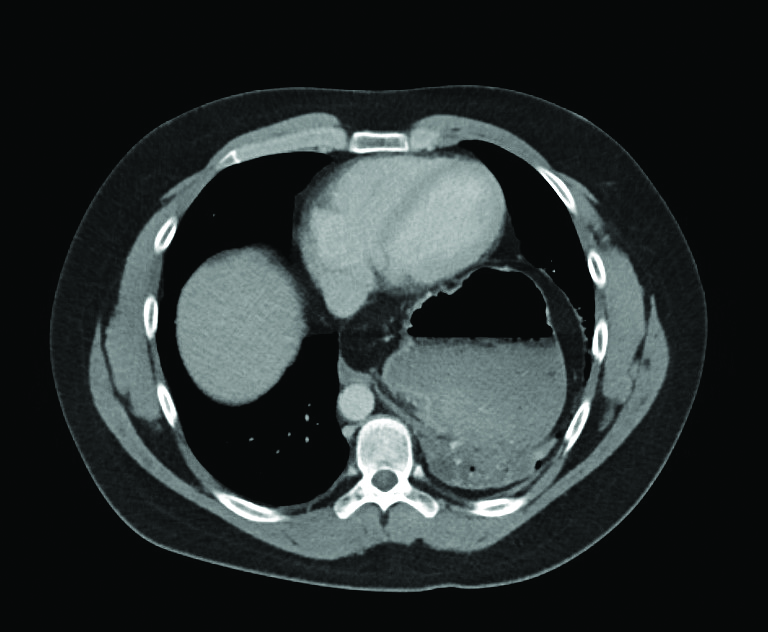
Figure 1. Initial CT abdomen showing a gastric volvulus within the large incarcerated hiatal hernia.
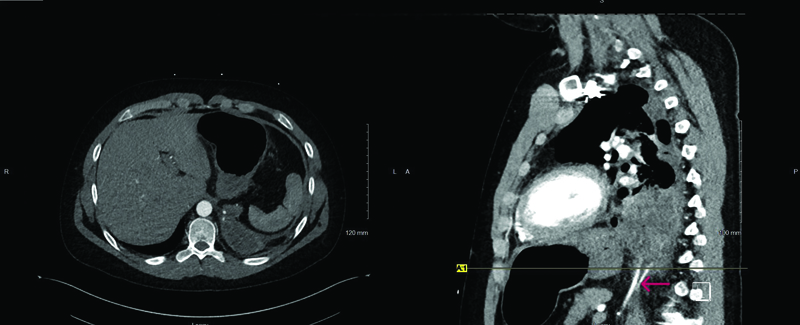
Figure 2. CT angiogram showing left lung pneumonia with complex effusion. Also shown are two arteries, one from the aorta, and one from the celiac trunk, both directly supplying the left lung base.
The patient underwent thoracotomy and decortication of the left lung. Due to significant adhesions from inflammation in the area, and potential risk of vascular injury and hemorrhage, the BPS was partially dissected from the diaphragm but not fully resected. Three days later, angiography of the feeding vessels was performed, and both feeder arteries were successfully embolized (Figure 3). During angiography, the venous drainage from the ILS was identified as flowing into the pulmonary veins, a characteristic of an intra-lobar BPS.4
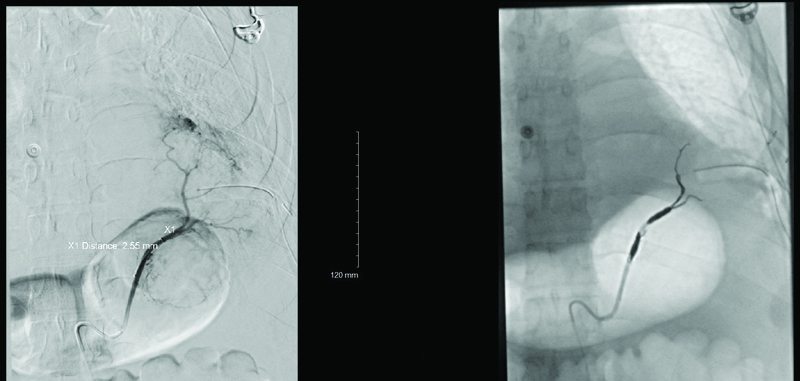
Figure 3. Angiography showing identification and successful embolization of the feeding vessels.
He returned to the operating room two days later and underwent re-exploration of the thoracotomy and resection of the intra-lobar BPS. Microbiologic work up including blood cultures and cultures of the resected lung tissue were unrevealing. Pathologic examination of the lung tissue revealed significant acute and chronic inflammation with focal necrosis. Over the following week, the patient made an unremarkable recovery and was discharged home on intravenous antimicrobials to complete a six-week course. He has since returned to work without residual dyspnea or other symptoms. Repeat imaging shows resolution of the complex effusion and pneumonia. Review of previous records showed that on multiple prior abdominal CT studies obtained during inflammatory bowel disease flare-ups, the patient had “chronic cystic changes” in the left lung base in the area where the sequestration was eventually identified.
DISCUSSION
Bronchopulmonary sequestration is a rare congenital abnormality. The majority of BPS are found in the posterior basal part of the left hemithorax.4 Intralobular sequestrations (ILS) usually present later in life and is associated with recurrent infection; extra lobular sequestrations (ELS) may manifest as cyanosis or an infection in neonates.8 Recurrent infections of ILS result in cystic changes and chronic inflammation.9 Both ILS and ELS are occasionally associated with diaphragmatic hernias.7
Our patient was found to have an ILS associated with a hiatal hernia complicated by an infection after repair of the hernia. Close attention should be paid to the vascular supply and drainage of the BPS. The outcome in our case appears to be curative following embolization and surgical resection, as is the case for most patients with BPS.10 Although surgical resection is considered even in asymptomatic cases, the risk of complications such as surgical infections, injury to the surrounding lung tissue and pleural space, and chylous leak is considerable. The decision to perform resection should weigh in the risk of surgical complications and comorbidities of individual patients.2
DISCLAIMERS
Informed consent was obtained from the patient prior to submission, and we intend to provide the patient with a copy of the publication.
REFERENCES
- Pryce DM. Lower accessory pulmonary artery with intralobar sequestration of lung; a report of seven cases. J Pathol Bacteriol1946 Jul;58(3):457–67.
- Alsumrain M, Ryu JH. Pulmonary sequestration in adults: a retrospective review of resected and unresected cases. BMC Pulm Med 2018;18:97. https://doi.org/10.1186/s12890-018-0663-z
- Correia-Pinto J, Gonzaga S, Huang Y, et al. Congenital lung lesions-underlying molecular mechanisms. Semin Pediatr Surg. 2010 Aug;19(3):171–9. doi: 10.1053/j.sempedsurg.2010.03.003
- Chakraborty RK, Modi P, Sharma S. Pulmonary Sequestration. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 24, 2023.
- Conran RM, Stocker JT. Extralobar sequestration with frequently associated congenital cystic adenomatoid malformation, type 2: report of 50 cases. Pediatr Dev Pathol 1999 Sep–Oct;2(5):454–63. doi: 10.1007/s100249900149
- Choo JY, Hwang J, Lee JH, et al. Bronchopulmonary foregut malformation presenting as extralobar pulmonary sequestration associated with a bronchogenic cyst: an unusual clinical and radiological feature in an adolescent patient. J Thorac Dis 2017 Jul;9(7):E632–E635. doi: 10.21037/jtd.2017.06.101
- Alhamad M, Anand D. Congenital diaphragmatic hernia with associated broncho-pulmonary sequestration: A report of two cases and a literature review. Journal of Neonatal-Perinatal Medicine 2024;17(1):123–31. doi:10.3233/NPM-230042
- Nair SP, Merry C, White A. Intralobar pulmonary sequestration in an adult: a case report. J Cardiothorac Surg. 2023 Jan 6;18(1):5. doi: 10.1186/s13019-023-02127-2
- Andrade CF, Ferreira HP, Fischer GB. Congenital lung malformations. J Bras Pneumol 2011 Mar–Apr;37(2):259–71. English, Portuguese. doi: 10.1590/s1806-37132011000200017
- Halkic N, Cuénoud PF, Corthésy ME, et al. Pulmonary sequestration: a review of 26 cases. Eur J Cardiothorac Surg. 1998;14(2):127–33. doi:10.1016/s1010-7940(98)00154-7
Article citation: Zaid AH, Abou-Yassine A. A rare case of bronchopulmonary sequestration associated with a hiatal hernia. The Southwest Journal of Medicine 2025; 13(57):40–43
From: Department of Pulmonary and Critical Care Medicine, Presbyterian Healthcare Services, Albuquerque, NM (AHZ, AA-Y)
Submitted: 7/9/2025
Accepted: 9/22/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.