CASE
A 77-year-old woman with a history of schizophrenia presented to the hospital with epigastric pain for two weeks associated with a 40-pound weight loss over the past six months. Physical examination showed thinning of the hairline (Figure 1A) and tenderness at the epigastrium. Laboratory tests showed iron deficiency anemia and hemoglobin 10.7 g/dL. Computed tomography of the abdomen with contrast showed abnormal gastric wall thickening and heterogenous mass within the stomach (Figure 1B and C). Esophagogastroduodenoscopy showed a large amount of hair in the gastric body and antrum along with one 15 mm clean based ulcer at the anterior wall of the stomach (Figure 2). Abiopsy from the gastric ulcer showed no evidence of malignancy. The patient was treated with pantoprazole twice daily, and the psychiatry team was consulted for evaluation of trichotillomania.
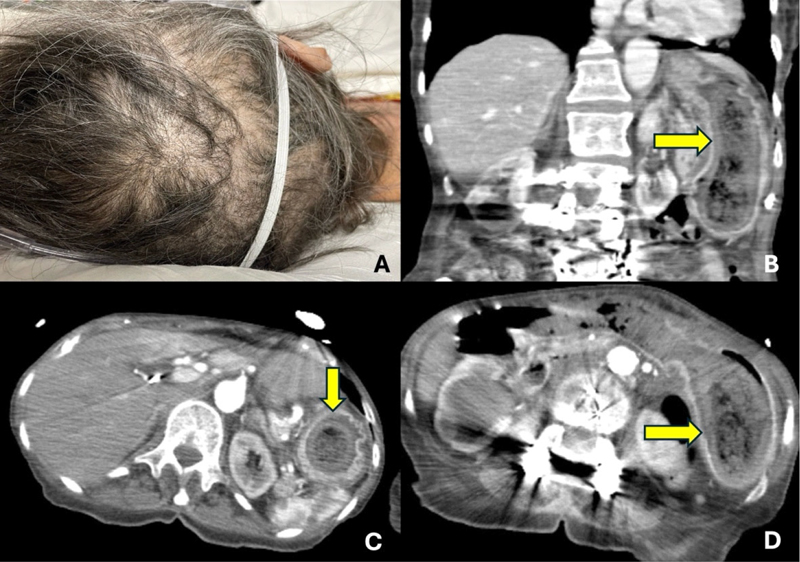
Figure 1. A: Physical examination shows patches of hair loss that are irregular in shape and broken hairs with different lengths. B: CT coronal plane shows the stomach distended (yellow arrow) with a large heterogenous mass lesion and show internal dense and air foci. C and D: CT axial plane shows a heterogenous mass in the stomach (yellow arrows) with air bubbles and internal dense foci. Gastric wall thickening was noted.
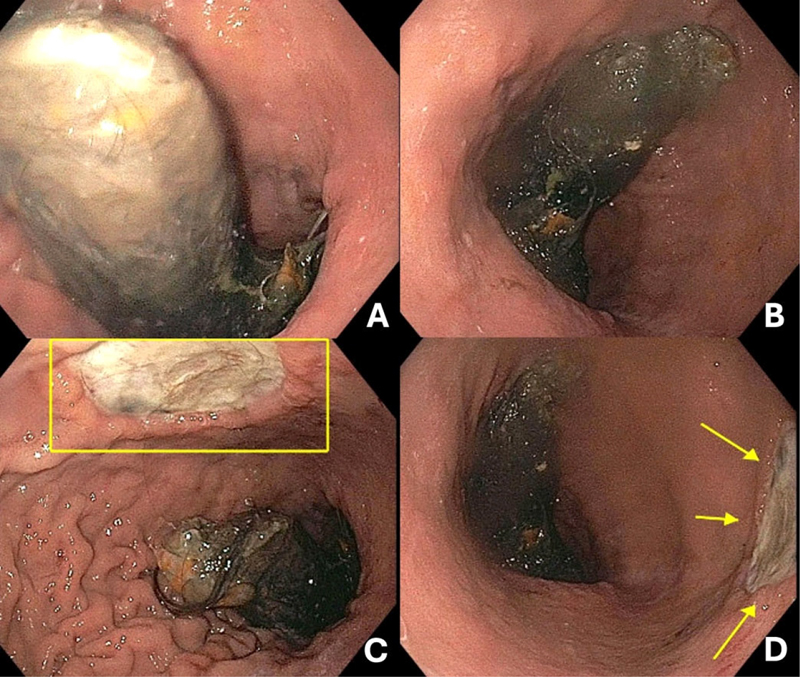
Figure 2. A and B: Esophagogastroduodenoscopy shows a large trichobezoar in the gastric body and antrum. C and D: One clean based ulcer measures 15 mm located at anterior wall of the stomach (yellow square and yellow arrow) and trichobezoar noted in the gastric body and the antrum.
DISCUSSION
Gastric trichobezoars are strongly associated with trichotillomania (prevalence 1 to 4%) with a female predominance.1 Symptoms often take months or years to develop. Symptoms include nausea, vomiting, and abdominal pain; many patients experience weight loss over time. Complications can be severe and include perforated gastric ulcer, gastric outlet obstruction, and protein-losing enteropathy.2 In this case, the patient’s abdominal pain is likely secondary to gastric ulcer which is caused by long-standing pressure on stomach lining from trichobezoar, which may reduce blood supply. Esophagogastroduodenoscopy is considered the gold standard for diagnosis. Treatment includes carbonated beverages due to an acidity effect, endoscopic removal, or surgical removal.2,3
Keywords: Trichobezoar, abdominal pain, gastric ulcer
REFERENCES
- Snorrason I, Ricketts EJ, Stein AT, et al. Sex differences in age at onset and presentation of trichotillomania and trichobezoar: a 120-year systematic review of cases. Child Psychiatry Hum Dev 2022;53(1):165–71. (In eng). DOI: 10.1007/s10578-020-01117-y.
- Kwon HJ, Park J. Treatment of large gastric trichobezoar in children: Two case reports and literature review. Medicine (Baltimore) 2023;102(16):e33589. (In eng). DOI: 10.1097/md.0000000000033589.
- Ladas SD, Kamberoglou D, Karamanolis G, et al. Systematic review: Coca-Cola can effectively dissolve gastric phytobezoars as a first-line treatment. Aliment Pharmacol Ther 2013;37(2):169–73. (In eng). DOI: 10.1111/apt.12141.
Article citation: Songtanin B, Evans J. Gastric ulcer from trichobezoar. The Southwest Journal of Medicine 2025;13(56):63–64
From: Division of Gastroenterology, Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, TX, USA; School of Medicine, Texas Tech University Health Sciences Center, Lubbock, TX, USA
Submitted: 5/26/2025
Accepted: 6/13/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.