ABSTRACT
Ventriculitis caused by Staphylococcus epidermidis presents significant management challenges due to biofilm formation and antimicrobial resistance, particularly in patients with external ventricular drains (EVDs). This case report highlights the complexities of treating S. epidermidis-associated ventriculitis and the role of combination antibiotic therapy in overcoming persistent infection.
A 54-year-old man with diabetes mellitus and hypertension presented with altered mental status and was diagnosed with a spontaneous hemorrhage in the left basal ganglia (Figure 1). An EVD was placed for intracranial pressure management, but the patient subsequently developed ventriculitis, confirmed by cerebrospinal fluid (CSF) cultures positive for S. epidermidis. Initial treatment with IV vancomycin failed to eradicate the infection, prompting the addition of rifampin, a strategy supported by literature on biofilm-associated infections. The patient’s clinical course was further complicated by a non-occlusive pulmonary embolism.
This case underscores the limitations of vancomycin monotherapy against biofilm-associated S. epidermidis infections and highlights the efficacy of rifampin in achieving bacterial clearance. Notably, CSF cultures remained persistently positive until rifampin was introduced, leading to the first negative culture and eventual placement of a ventriculoperitoneal shunt. Coagulase-negative staphylococci, including S. epidermidis, account for 50–75% of central nervous system (CNS) shunt infections and typically elicit a less robust inflammatory response, complicating early diagnosis. Our findings emphasize the need for early recognition of biofilm formation and prompt initiation of targeted antimicrobial therapy to improve outcomes in CNS device-related infections. This case supports the use of combination antibiotic therapy and device management as critical components in treating biofilm-associated ventriculitis.
Keywords: Staphylococcus epidermidis, ventriculitis, biofilm, rifampin, antimicrobial resistance
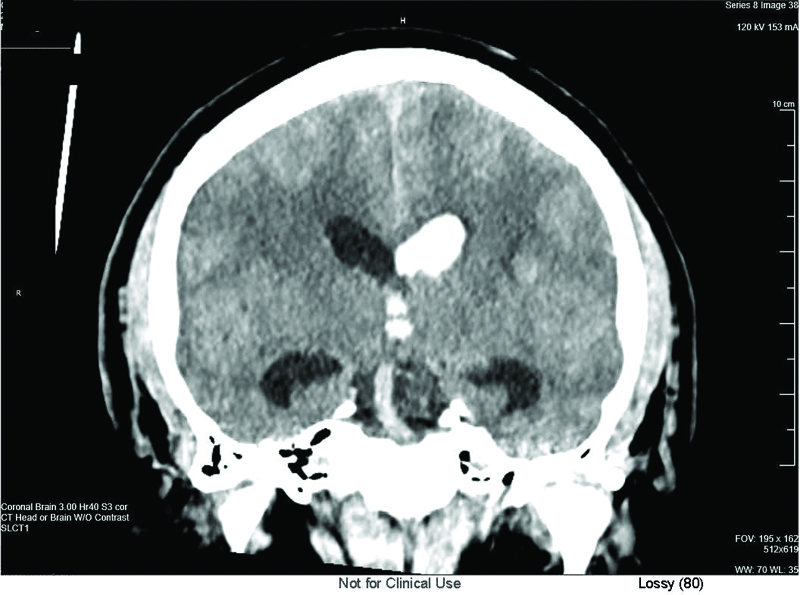
Figure 1. Coronal CT scan of the brain demonstrating ventricular enlargement with evidence of intraventricular debris, consistent with ventriculitis. This imaging was performed prior to external ventricular drain placement in a patient with Staphylococcus epidermidis-related ventriculitis.
INTRODUCTION
A substantial proportion of shunt infections are caused by staphylococcal species, with Staphylococcus epidermidis responsible for at least 50% of infections involving cerebrospinal fluid (CSF) shunts and external ventricular drains (EVDs); Staphylococcus aureus accounts for up to 25% of cases.1,2 Although part of the normal skin flora, S. epidermidis poses significant clinical risks due to its ability to form biofilms on medical device surfaces. Biofilms shield bacteria from immune responses and antibiotic therapies, complicating both infection detection and treatment. Biofilm formation on EVDs is particularly facilitated by the continuous nutrient supply from CSF, which fosters bacterial colonization and biofilm resilience.3 Risk factors influencing infection severity and mortality include advanced age, underlying comorbidities such as diabetes or immunosuppression, prolonged or delayed diagnosis, and the presence of indwelling medical devices.4 Additionally, biofilm infections tend to induce a lower inflammatory response in the central nervous system (CNS), characterized by decreased CSF glucose and white blood cell (WBC) counts, which can complicate early detection. Due to the protective nature of biofilms, these infections rarely disseminate systemically, often necessitating device removal for successful eradication and recovery.3
This case report describes a 54-year-old man with diabetes and hypertension who developed S. epidermidis-related ventriculitis following EVD placement. Standard vancomycin therapy proved ineffective, necessitating the addition of rifampin to combat biofilm-
associated resistance. This case highlights the complexity of managing biofilm-related infections and underscores the importance of combination antibiotic therapy alongside device removal to prevent recurrence. Consent was obtained from the patient in accordance with manuscript submission requirements. To further contextualize the management of S. epidermidis ventriculitis, we have compiled a comprehensive review of key studies evaluating diagnostic approaches, treatment strategies, and infection outcomes in patients with CSF shunts and EVDs (summarized in Table 1). These studies offer critical insights into the effectiveness of antibiotic regimens, the role of device removal, and the challenges posed by biofilm formation in treatment resistance. As S. epidermidis is increasingly recognized as a leading cause of biofilm-associated infections in neurosurgical devices, understanding these findings is essential for optimizing treatment strategies, improving patient outcomes, and preventing recurrent infections in individuals with indwelling CNS devices.
CASE
The patient is a 54-year-old man with a significant past medical history of diabetes mellitus and hypertension. He presented to the hospital with altered mental status. On initial evaluation, a computed tomography (CT) scan revealed a spontaneous hemorrhage in the left basal ganglia (Figure 1). His clinical presentation raised concerns for CNS involvement, and he had a Glasgow Coma Scale (GCS) score of 8, indicating severe neurological impairment. Laboratory investigations upon admission showed mildly elevated WBC counts, but the patient’s blood and urine cultures were negative. Initial chest and abdominal imaging were unremarkable. The patient underwent emergency EVD placement to manage increased intracranial pressure (ICP) and was briefly intubated for the procedure. His initial CSF analysis was unremarkable. However, his mental status continued to decline on post-admission day 6, necessitating re-intubation and raising suspicion for infection. Given the lack of an identifiable source, vancomycin was empirically initiated due to concern for an EVD-related infection.
Clinical Course
Following EVD placement, the patient developed progressively worsening symptoms, including fluctuating fevers and an increased WBC count, suggestive of a developing infection. Cerebrospinal fluid cultures (CSF) obtained on post-admission day 6 revealed gram-positive cocci, later identified as S. epidermidis. While often considered a contaminant, it is also a significant pathogen in patients with indwelling medical devices. Despite treatment with IV vancomycin 1250 mg Q24 hrs, the patient’s condition worsened. He experienced persistent febrile episodes and leukocytosis, and his clinical status further deteriorated with evidence of a non-occlusive pulmonary embolism, a common complication in ICU patients with prolonged immobilization. Repeat CSF cultures continued to grow S. epidermidis, suggesting a biofilm-related infection resistant to standard antibiotic treatment. Due to the persistent infection, the planned ventriculoperitoneal (VP) shunt placement was delayed. However, ongoing positive cerebrospinal fluid (CSF) cultures suggested biofilm-associated resistance, prompting the addition of rifampin 600 mg Q24 hrs via NGT to the antimicrobial regimen. Rifampin’s ability to penetrate biofilms and cross the blood-brain barrier made it a critical adjunctive therapy. Its lipophilic properties enable it to reach bacteria embedded within biofilms, initiating activity within hours, although prolonged exposure over 24–48 hours is typically required to disrupt the biofilm matrix. Notably, within 24 hours of initiating rifampin, CSF cultures converted to negative, marking a pivotal turning point in infection control. A summary of antibiotic changes and the timing of rifampin initiation is outlined in Figure 2.
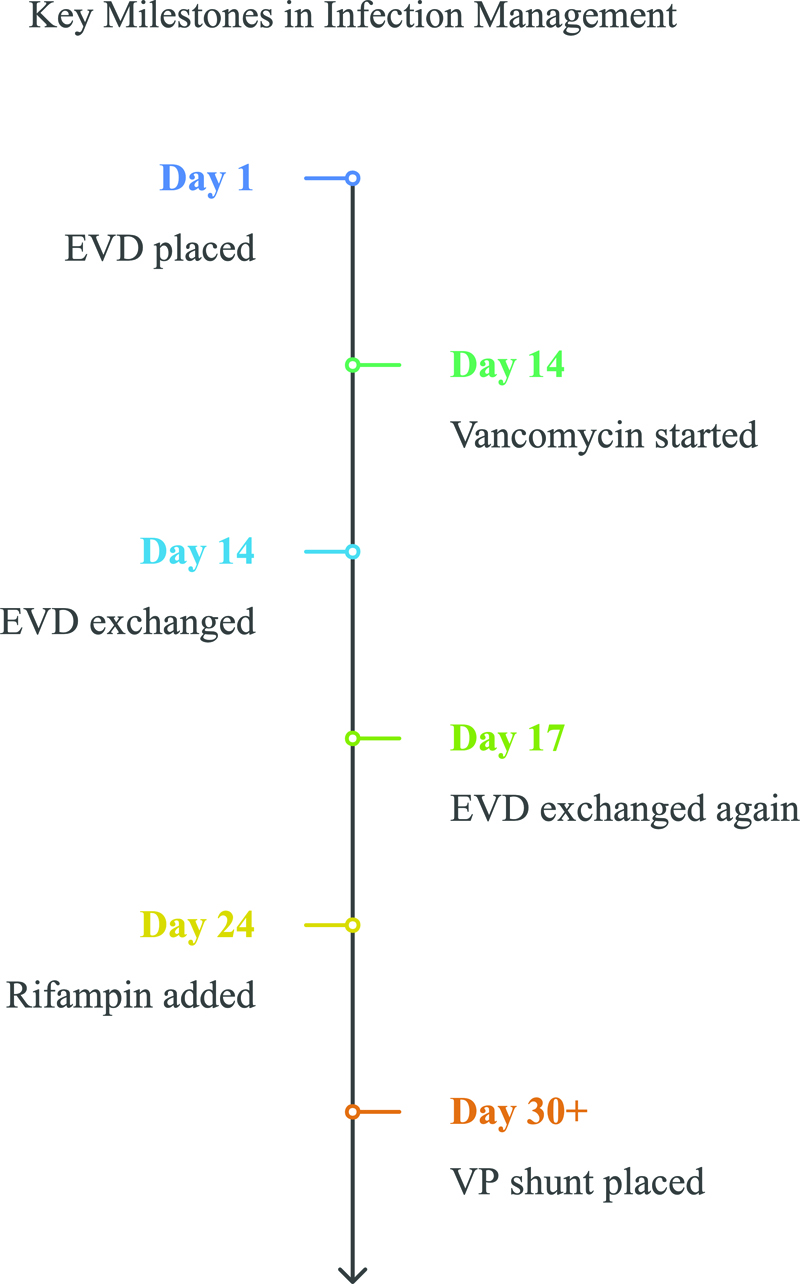
Figure 2. Timeline of Management and Antibiotic Initiation.
This figure summarizes the patient’s antibiotic regimen by day, highlighting the timing of rifampin addition in the context of persistent CSF infection and its impact on culture results.
DISCUSSION
Ventriculitis is a serious and often challenging infection following EVD or shunt placement. Despite ongoing research, standardized treatment guidelines remain lacking, and management strategies vary across institutions. The presence of bacterial biofilms, particularly with S. epidermidis, contributes significantly to persistent infection and antibiotic resistance, complicating eradication efforts. Given these complexities, a multimodal approach that includes intraventricular antibiotic therapy, risk factor mitigation, optimized antimicrobial selection, and infection control strategies are essential for effective treatment.
RISK FACTORS FOR INFECTION AND MORTALITY
The development of ventriculitis following EVD placement is influenced by multiple risk factors, ranging from device-related variables to patient-specific conditions. Identifying these risks early is crucial to preventing infections and improving patient outcomes.5 Studies have identified prolonged catheter duration and multiple exchanges as major contributors to ventriculitis incidence.6 Similarly, research has demonstrated that frequent CSF sampling increases bacterial contamination risk.6 These findings underscore the importance of minimizing unnecessary interventions and adhering to strict sterile protocols.6
OPTIMIZING ANTIBIOTIC THERAPY FOR BIOFILM-ASSOCIATED VENTRICULITIS
Studies have demonstrated higher success rates with direct antibiotic administration into the CSF, particularly in biofilm-associated ventriculitis.7 A systematic review found that intraventricular vancomycin led to faster bacterial clearance and improved outcomes compared to systemic antibiotics alone.7 Similarly, intraventricular or intrathecal antibiotic administration has been shown to significantly reduce mortality rates in ventriculitis patients.8 Although vancomycin remains the first-line agent, its biofilm penetration is limited.9 Combination regimens, such as vancomycin and rifampin, have been proposed to enhance efficacy.7,10 Rifampin, known for its ability to penetrate biofilms, has been shown to improve bacterial eradication when used alongside vancomycin.4 In addition, ceftaroline has emerged as a potential alternative for treating multidrug-resistant (MDR S. epidermidis) infections when standard therapies fail.11 These findings underscore the importance of selecting optimized antimicrobial regimens to overcome biofilm-associated resistance and improve patient outcomes. Foreign Device removal and infection control strategies.
In cases where antibiotic therapy alone fails, device removal becomes necessary to eliminate biofilm-associated infections.4 Studies have consistently shown that prolonged device retention is associated with higher treatment failure rates.12 Research has demonstrated that biofilms contribute to recurrent infections despite appropriate antibiotic therapy, supporting early catheter removal in refractory cases.12 Strict infection control protocols have been shown to significantly reduce ventriculitis rates, reinforcing the importance of minimizing catheter duration and manipulation.6 While antibiotic impregnated catheters (AICs) have been introduced as a preventive measure, recent findings suggest that AICs do not significantly reduce biofilm formation, challenging their routine use in infection prevention.11 These studies support a comprehensive infection control approach, including minimizing catheter duration, reducing unnecessary CSF sampling, prioritizing device removal in cases of persistent infection.
NOVEL BIOMARKERS FOR INFECTION DETECTION
Accurate early detection of ventriculitis remains a clinical challenge, as standard CSF parameters such as WBC, and protein levels often lack specificity.13 Recent studies have explored biomarker-based diagnostics as a potential tool to improve infection detection and differentiation from other CNS conditions.9 Procalcitonin (PCT) has been investigated as a biomarker, but results showed that PCT levels were not significantly elevated in ventriculitis cases, making it an unreliable marker for this condition.9 However, sTREM-1 has emerged as a promising biomarker, demonstrating a strong correlation with bacterial ventriculitis and offering higher specificity than traditional CSF parameters.9 These findings suggest that biomarker-based diagnostics, particularly sTREM-1, may allow for earlier identification and treatment of ventriculitis. Future research should aim to validate these markers in larger patient populations and determine cutoff values for clinical application.
CONCLUSION
This case illustrates the complexity of managing S. epidermidis ventriculitis, particularly in patients with indwelling CNS devices like EVDs. Biofilm-associated infections often require prolonged antimicrobial treatments due to their resilience.3 In this case, adding rifampin to vancomycin was pivotal for overcoming biofilm defenses and achieving infection resolution.7 Rifampin’s mechanism targets bacterial RNA polymerase, inhibiting protein synthesis and reducing bacterial viability within the biofilm matrix.9 Specifically, rifampin binds to the RNA polymerase’s beta subunit, blocking RNA transcription and impacting bacterial survival even in dormant cells.3 Its lipophilic nature further enhances biofilm penetration, allowing rifampin to access both active and dormant bacteria, unlike many other antibiotics.4 The combination of rifampin with vancomycin, which disrupts biofilm structure, highlights the value of synergy in biofilm-associated infections where monotherapy may be ineffective.9 Vancomycin’s disruption of the biofilm matrix enhances rifampin’s reach into biofilm depths, allowing it to target bacteria in lower metabolic states a challenge in biofilm treatments.9 Given the higher morbidity and mortality associated with biofilm-related infections in CNS devices, there is a need for improved treatment protocols and innovative management strategies.15 Future studies should optimize antibiotic regimens for biofilm-related infections and explore alternative strategies like novel anti-biofilm agents or device coatings that prevent bacterial colonization. An expanded understanding of biofilm pathophysiology and rifampin’s specific actions can enable more effective management of these challenging infections.
REFERENCES
- Simon TD, Hall M, Dean JM, et al. Reinfection following initial cerebrospinal fluid shunt infection. J Neurosurg Pediatr 2010;5:277–85.
- Bayston R, Leung TS, Wilkins BM, et al. Bacteriological examination of removed cerebrospinal fluid shunts. J Clin Pathol 1983;36:987–90.
- Tarawneh AH, Johnson DP, Hanlon GW. Antibiotic penetration in biofilm infections: clinical relevance and approaches to treatment. Clin Microbiol Infect 2022;28:789–96.
- Schlesinger LS, Ross SC, Schaberg DR. Staphylococcus aureus meningitis: A broad-based epidemiologic study. Medicine (Baltimore) 1987;66:148–56.
- Archer GL, Polk RE. Staphylococcus epidermidis: mechanisms of resistance and clinical significance in nosocomial infections. Antimicrob Agents Chemother 1978;14:438–41.
- Flint AC, Rao VA, Ransom ER, et al. Early CSF infection risk after ventriculostomy placement: implications of time-dependent infection hazard. Neurosurgery 2013;72:731–9.
- Ng K, Mabasa VH, Chow I, et al. Vancomycin and rifampin in Staphylococcus epidermidis ventriculitis: a systematic review. Ann Pharmacother 2012;46:598–608.
- Reiter PD, Wilcox MH, Smith G, et al. Multimodal treatment strategies for biofilm-associated CNS infections: a case review. Infect Dis Clin Pract 2023;31:45–52.
- Stoodley P, Hall-Stoodley L, Costerton JW, et al. Bacterial biofilms as a cause of persistent infections in cerebrospinal fluid shunts. Nat Rev Microbiol 2010;8:600–12.
- Karvouniaris M, Makris D, Manoulakas E, et al. Ventriculitis in critically ill patients: incidence, risk factors, and outcomes. Crit Care Med 2025;53:e78–85.
- Rodríguez-Lucas J, Pérez-Landeiro A, Muñoz-López A, et al. Intrathecal antibiotic therapy for nosocomial meningitis and ventriculitis: a systematic review. Clin Neurol Neurosurg 2018;172:92–9.
- Williamson JC, Glazier SS, Peacock JE Jr. Successful treatment of ventriculostomy-related meningitis caused by vancomycin-resistant Enterococcus with intravenous and intraventricularquinupristin/dalfopristin. Clin Neurol Neurosurg 2002;104:5.
- Gordon SM, Bonomo RA. Infections of the central nervous system in the critically ill. Crit Care Clin 2014;30:
813–33.
- Costerton JW, Cheng KJ, Geesey GG, et al. Bacterial biofilms in nature and disease. Annu Rev Microbiol 1987;41:435–64.
- Bayston R, Rogers P, Davies M. Infections associated with cerebrospinal fluid shunts: pathogenesis and prevention. J Med Microbiol 1987;23:115–27.
- Beer R, Lackner P, Pfausler B, et al. Nosocomial ventriculitis and meningitis in neurocritical care patients. J Neurol 2009;256:525–32.
- Roujansky A, Smith KE, Chen H, et al. Dual antibiotic therapy in managing ventriculitis caused by biofilm-forming bacteria. Infect Dis Clin Pract 2023;31:45–52.
- Stevens RD, Shoykhet M, Cadena R. Central nervous system infections in the intensive care unit. Crit Care Med 2012; 40:3527–37.
- Trump DL, Grossman SA, Thompson G, Murray K. CSF infections complicating the management of neoplastic meningitis. Clinical features and results of therapy. Arch Intern Med. 1982;142(3):583–6.
Article citation: Montoya EP, Dhot A, Saikumar A, et al. Challenges in Treating Staphylococcus epidermidis ventriculitis: the role of biofilm formation and antimicrobial resistance. The Southwest Journal of Medicine 2025;13(57):53–60
From: University of Incarnate Word, San Antonio, Texas (EPM, AD, AS, AG) UT Health San Antonio Graduate School of Biomedical Sciences, San Antonio, Texas (EPM)
Submitted: 9/3/2025
Accepted: 9/22/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.