CASE
A 41-year-old woman with a history of classic 21-hydroxylase deficiency congenital adrenal hyperplasia, diagnosed in childhood and associated with male reproductive organs, presented after several years without follow-up or medical therapy. She arrived with abdominal pain and anuria, and was in mixed shock from adrenal crisis and septic shock secondary to Escherichia coli pyelonephritis. Initial imaging showed profound enlargement of her bilateral adrenal glands (Figure 1A and B). During hospitalization, she required vasopressor support and renal replacement therapy. Broad-spectrum antibiotics with cefepime were initiated and subsequently narrowed to ceftriaxone, along with stress-dose corticosteroids, resulting in clinical improvement. Hormonal evaluation revealed no evidence of adrenal hypersecretion. She was discharged on hydrocortisone, but declared to have end-stage renal disease requiring ongoing dialysis. Outpatient follow-up with endocrinology and endocrine surgery was arranged to evaluate for bilateral adrenalectomy.
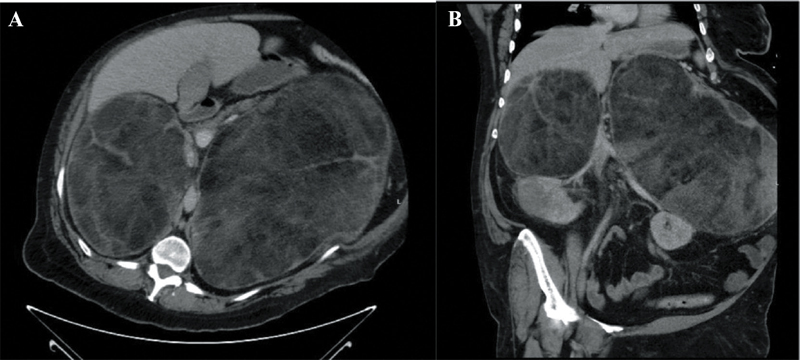
Figure 1. A: Contrast-enhanced computed tomography of the abdomen and pelvis in the axial view revealing large bilateral adrenal masses containing macroscopic fat and soft tissue components. The right adrenal lesion measured 13.6 × 19.2 × 15.6 cm, while the left measured 28.3 × 20.9 × 29.6 cm. These findings were most consistent with adrenal myelolipomas; however, retroperitoneal sarcoma and lymphoma were considered as part of the differential diagnosis. B: Coronal view of the large bilateral adrenal mass.
DISCUSSION
Initial cross-sectional imaging demonstrated marked, bilateral adrenal enlargement, a finding that can occur in patients with longstanding untreated congenital adrenal hyperplasia (CAH) due to chronic ACTH stimulation. In this patient, the images raised concern for adrenal myelolipomas, benign tumors commonly associated with CAH and characterized radiographically by the presence of macroscopic fat intermixed with soft-tissue elements.1,2 Myelolipomas are typically nonfunctioning but can attain substantial size, leading to mass effect, abdominal pain, or hemorrhage.1,2 The bilateral nature and degree of enlargement in this case are consistent with the recognized propensity of CAH patients to develop multiple and large adrenal myelolipomas, highlighting the importance of imaging in guiding both acute management and long-term surgical planning.
Keywords: Congenital adrenal hyperplasia, adrenal myelolipoma
REFERENCES
- Calissendorff J, Juhlin CC, Sunlin A, et al. Adrenal myelolipomas. The Lancet Diabetes & Endocrinology 2022;9(11):767–75. DOI:10.1016/S2213-8587(21)00178-9
- Rao K, Kenney PJ, Wagner B, et al. Imaging and pathologic features of myelolipoma. Radiographics: a review publication of the Radiological Society of North America, Inc. 1997;17(6):1373–85. DOI:10.1148/radiographics.17.6.
Article citation: Evans A. Profound adrenal enlargement in 21-hydroxylase-deficiencye. The Southwest Journal of Medicine 2025;13(57):72–73
From: Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas (AE)
Submitted: 9/1/2025
Accepted: 9/15/2025
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.