Abstract
The association between hospital teaching status and in-hospital outcomes among patients with type 2 myocardial infarction in the United States
Panat Yanpiset MD, Chanokporn Puchongmart MD, Diego Cruz MD, Cristian Castillo Rodriguez MD, Joseph Sena MD, Sireethorn Wonghanchai MD, Varote Shotelersuk MD, Ben Thiravetyan MD
Corresponding author: Ben Thiravetyan
Contact Information: Ben.Thriavetyan@ttuhsc.edu
DOI: 10.12746/swjm.v14i59.1625
ABSTRACT
Background: Type 2 myocardial infarction (T2MI) is characterized by an imbalance between myocardial oxygen supply and demand in the absence of acute coronary obstruction. The current lack of clear diagnostic and management guidelines for T2MI could lead to disparities in management and outcomes across different hospital settings.
Methods: We performed a retrospective analysis using the National Inpatient Sample from 2017 to 2022, identifying adult hospitalizations with T2MI. Hospitals were categorized as rural, urban non-teaching, or urban teaching. The primary outcome was in-hospital mortality. Survey-weighted logistic regression was used to identify predictors of mortality.
Results: Among all hospitalizations for T2MI, 8.3% occurred in rural hospitals, 16.3% in urban non-teaching hospitals, and 75.4% in urban teaching hospitals. Patients at urban teaching hospitals were slightly younger but had higher rates of comorbidities. In-hospital mortality was significantly greater in urban teaching hospitals (10.5% vs. 9.3% and 8.8% in urban non-teaching and rural hospitals, respectively). After adjustment, urban teaching hospital status remained an independent predictor of mortality.
Conclusion: Patients with T2MI treated at urban teaching hospitals were associated with increased mortality, length of stay, and total hospital charges. Teaching hospital status was also found to be an independent risk factor for in-hospital mortality.
Keywords: Myocardial infarction; type 2 myocardial infarction; mortality; teaching hospital
INTRODUCTION
Type 2 myocardial infarction (T2MI) is a subtype of myocardial infarction that results from an imbalance between myocardial oxygen supply and demand, rather than acute plaque rupture. It represents a growing subset of myocardial infarction cases. Compared to patients with type 1 myocardial infarction, patients with T2MI are generally older, have a greater burden of comorbidities, and are at increased risk for adverse outcomes, including in-hospital mortality.1 Despite its clinical relevance, T2MI remains under-investigated, and standardized management strategies are lacking.1
Hospital-level factors, such as teaching status, may influence clinical outcomes in patients with T2MI due to their ability to treat underlying illnesses. Teaching hospitals often benefit from greater subspecialty availability, advanced diagnostic capabilities, and academic infrastructure, potentially contributing to better outcomes.2 In contrast, rural and urban non-teaching hospitals may face resource limitations, including reduced access to cardiology expertise or procedural interventions. While some studies have reported lower mortality associated with teaching hospital status in general, others have shown slightly higher mortality rates for specific emergent procedures performed in teaching hospitals.3
Based on the lack of a gold standard in diagnosis, risk stratification, and treatment guidelines.1 T2MI could further complicate management and may contribute to variation in care across hospital settings. This study aims to examine differences in in-hospital outcomes among patients with T2MI across hospital settings, specifically rural, urban non-teaching, and urban teaching hospitals. By assessing variation in patients’ characteristics, primary payer types, and co-morbidities to determine whether disparities in diagnosis and management exist based on hospital teaching status and location.
METHOD
We conducted a retrospective analysis study using data from the National Inpatient Sample (NIS) from 2017 to 2022. The NIS is part of the Healthcare Cost and Utilization Project (HCUP) and is the largest publicly available all-payer inpatient database in the United States, containing a 20% stratified sample of discharges from community hospitals.
We included adult patients aged ≥18 years who were hospitalized with a principal or secondary diagnosis of type 2 myocardial infarction (T2MI), identified using the ICD-10-CM diagnosis code I21.A1, “type 2 myocardial infarction”. Patients with missing data for key variables, e.g., age, sex, mortality, race, length of stay, or total charges, were excluded from the analysis.
The hospital’s teaching status was obtained from the American Hospital Association Annual Survey of Hospitals. A metropolitan statistical area is considered urban, and a non-metropolitan statistical area is rural. Teaching hospitals have an American Medical Association-approved residency program or are members of the Council of Teaching Hospitals. Patients’ comorbidities were measured using individual Elixhauser comorbidity flags defined by HCUP software.
OUTCOMES
The primary outcome was in-hospital mortality. Secondary outcomes included length of stay (LOS) and total hospital charges (THC). THC was reported in U.S. dollars and adjusted for inflation to 2022 using the Consumer Price Index, as provided by the U.S. Bureau of Labor Statistics. Charges from 2017 to 2021 were converted to 2022 dollars using year-specific inflation factors.
STATISTICAL ANALYSIS
All analyses were conducted using Stata version 18.0 (StataCorp, College Station, TX). Descriptive statistics summarized baseline characteristics between T2MI patients. Continuous variables were reported as means ± standard deviations or medians with interquartile ranges, as appropriate. Categorical variables were summarized as weighted percentages. Characteristics between patients across hospital types were compared using design-based F tests from a survey-adjusted chi-square test. Continuous variables were reported as means with standard deviations or medians with interquartile ranges and compared using survey-weighted linear regression as appropriate. Logistic regression was used to estimate the association between hospital teaching status and in-hospital mortality. Adjusted odds ratios (aORs) and 95% confidence intervals (CI) were reported. A two-sided p-value <0.05 was considered statistically significant.
RESULTS
From 2017 to 2022, a total of 2,034,364 patients were included in the study. Baseline characteristics are shown in Table 1. The distribution across hospital types was 8.3% in rural hospitals, 16.3% in urban non-teaching hospitals, and 75.4% in urban teaching hospitals, as illustrated in Figure 1. Patients admitted to rural hospitals were slightly older compared to those in urban non-teaching and urban teaching hospitals (mean age 72.1 vs. 71.7 vs. 70.1 years, respectively; p < 0.01). The majority of patients were White, with a higher proportion observed in rural hospitals than in urban non-teaching and urban teaching hospitals (87.6% vs. 72.9% vs. 64.2%, respectively).
Table 1. Baseline Characteristics of Patients Hospitalized with T2mi by Hospital Location and Teaching Status
| Characteristics |
Rural (N = 169,450) |
Urban Non-Teaching (N = 331,040) |
Urban Teaching (N = 1,533,874) |
p-value |
| Prevalence, % |
8.3% |
16.3% |
75.4% |
– |
| Age, year |
72.1 ± 0.1 |
71.7 ± 0.1 |
70.1 ± 0.1 |
<0.01 |
| Female, % |
48.8% |
47.7% |
46.7% |
<0.01 |
| Race, % |
|
|
|
<0.01 |
| White |
87.6 |
72.9 |
64.2 |
|
| Black |
7.6 |
12.6 |
19.4 |
|
| Hispanic |
2.1 |
8.8 |
9.9 |
|
| Asian/Pacific Islander |
0.5 |
2.8 |
3.0 |
|
| Native American |
1.5 |
0.5 |
0.7 |
|
| Other |
0.7 |
2.5 |
2.9 |
|
| Comorbidities, % |
|
|
|
|
| Hypertension |
80.5 |
81.8 |
81.9 |
<0.01 |
| Diabetes |
40.8 |
40.7 |
41.9 |
<0.01 |
| Congestive Heart Failure |
56.8 |
57.1 |
58.1 |
<0.01 |
| Cardiac Arrhythmias |
48.3 |
48.1 |
47.8 |
0.46 |
| Valvular Heart Disease |
18.1 |
19.3 |
18.9 |
0.04 |
| Chronic pulmonary disease |
39.4 |
33.1 |
30.8 |
<0.01 |
| Renal failure |
37.8 |
39.3 |
40.6 |
<0.01 |
| Liver disease |
7.5 |
8.5 |
9.9 |
<0.01 |
| Cancer |
7.1 |
7.3 |
8.5 |
<0.01 |
| Coagulopathy |
11.0 |
13.3 |
14.9 |
<0.01 |
| Obesity |
19.4 |
19.3 |
19.1 |
0.52 |
| Alcohol abuse |
4.9 |
5.3 |
5.8 |
<0.01 |
| Drug abuse |
5.6 |
6.2 |
7.1 |
<0.01 |
| Primary Payer, % |
|
|
|
<0.01 |
| Medicare |
73.7 |
72.3 |
69.1 |
|
| Medicaid |
8.7 |
8.9 |
12.0 |
|
| Private Insurance |
11.5 |
12.8 |
13.3 |
|
| Self-Pay |
2.3 |
3.1 |
1.3 |
|
| Percutaneous Coronary Intervention, % |
0.9 |
1.1 |
1.5 |
<0.01 |
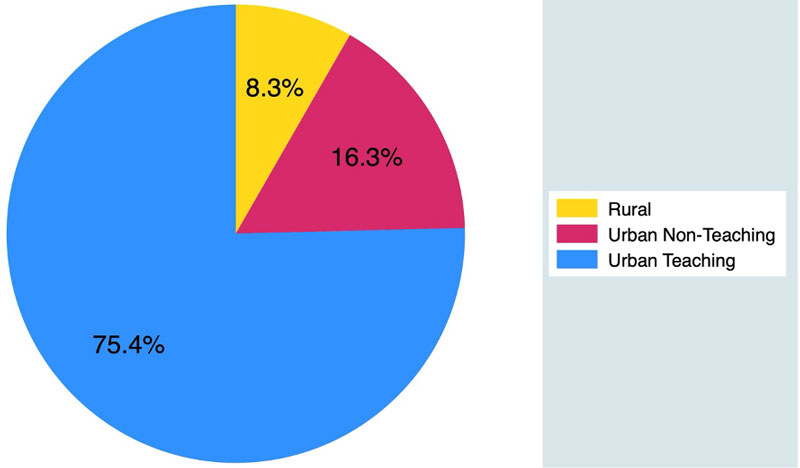
Figure 1 Distribution of patients hospitalized with T2MI by hospital location and teaching status.
The most common comorbidities across all hospital types were hypertension, congestive heart failure, cardiac arrhythmias, and diabetes mellitus. Patients treated at urban teaching hospitals tended to have a higher burden of severe comorbidities, including a greater prevalence of hypertension, congestive heart failure, diabetes, renal failure, liver disease, cancer, coagulopathy, alcohol abuse, and drug abuse. In contrast, diseases such as chronic pulmonary disease were lower in an urban teaching hospital. Rates of percutaneous coronary intervention (PCI) were low among all three groups. However, it was observed to be the highest among the urban teaching hospitals (0.9% vs. 1.1% vs. 1.5% in rural, urban non-teaching, and urban teaching hospitals, respectively; p < 0.01).
In unadjusted analysis, the in-hospital mortality outcome was found to be highest in urban teaching hospitals as demonstrated in Table 2 (8.8% vs. 9.3% vs. 10.5% in rural, urban non-teaching, and urban teaching hospitals, respectively; p < 0.01). Similarly, LOS and THG were found to be greater in the urban teaching group (4 vs. 5 vs. 5 days in rural, urban non-teaching, and urban teaching hospitals, respectively; p < 0.01) and ($39,185 vs. $60,378 vs. $65,854 in rural, urban non-teaching, and urban teaching hospitals, respectively; p < 0.01).
Table 2. In-Hospital Outcomes by Hospital Location and Teaching Status
| Outcomes |
Rural |
Urban Non-Teaching |
Urban Teaching |
p-value |
| Primary Outcome |
| In-hospital mortality, % |
8.8 |
9.3 |
10.1 |
<0.01 |
| Secondary Outcomes |
| LOS, days (IQR) |
4 (3,7) |
5 (3,8) |
5 (3,10) |
<0.01 |
| Total Hospital Charges $, (IQR) |
$39,185 ($23,270–$69,759) |
$60,378 ($33,850–$113,232) |
$65,854 ($35,693–$130,762) |
<0.01 |
In the adjusted model, hospital teaching status was found to be an independent factor for an increase in in-hospital mortality (aOR 1.06, 95% CI: 1.04–1.08). Older age was also associated with increased mortality (aOR 1.02, 95% CI: 1.02–1.02). Hispanic and Asian/Pacific Islander were found to be at risk of increased hospital mortality compared to the white population; Hispanic (aOR 1.13, 95% CI: 1.09–1.17) and Asian/Pacific Islander (aOR 1.09, 95% CI: 1.02–1.16). Comorbidities associated with increased mortality were liver disease (aOR 3.01, 95% CI: 2.92–3.10, coagulopathy (aOR 2.10, 95% CI: 2.04–2.15), cancer (aOR 1.53, 95% CI: 1.48–1.58), and congestive heart failure (aOR 1.06, 95% CI: 1.04–1.08), whereas hypertension, diabetes, valvular heart disease, alcohol abuse and drug abuse were associated with decreased odds for in-hospital mortality (Table 3 and Figure 2). Primary Payers were mostly found to be similar to Medicare, except for self-pay, which was associated with increased mortality (aOR 1.14, 95% CI: 1.06–1.22).
Table 3. Adjusted Odds Ratios for Predictors of In-Hospital Mortality
| Predictors |
aOR (95% CI) |
p-value |
| Hospital Teaching Status |
1.06 (1.04–1.08) |
<0.01 |
| Age, year |
1.02 (1.02–1.02) |
<0.01 |
| Female (vs Male) |
0.89 (0.87–0.91) |
<0.01 |
| Race (vs White) |
| Black |
1.01 (0.98–1.04) |
0.47 |
| Hispanic |
1.13 (1.09–1.17) |
<0.01 |
| Asian/Pacific Islander |
1.09 (1.02–1.16) |
0.01 |
| Native American |
1.10 (0.97–1.24) |
0.14 |
| Other |
1.23 (1.16–1.31) |
<0.01 |
| Comorbidities, % |
| Hypertension |
0.55 (0.54–0.57) |
<0.01 |
| Diabetes Mellitus |
0.92 (0.90–0.94) |
<0.01 |
| Congestive Heart Failure |
1.06 (1.04–1.08) |
<0.01 |
| Valvular Heart Disease |
0.66 (0.64–0.68) |
<0.01 |
| Chronic Pulmonary Disease |
0.99 (0.97–1.02) |
0.60 |
| Renal Failure |
1.01 (0.99–1.04) |
0.29 |
| Liver Disease |
3.01 (2.92–3.10) |
<0.01 |
| Cancer |
1.53 (1.48–1.58) |
<0.01 |
| Coagulopathy |
2.10 (2.04–2.15) |
<0.01 |
| Alcohol Abuse |
0.60 (0.57–0.64) |
<0.01 |
| Drug Abuse |
0.63 (0.60–0.67) |
<0.01 |
| Primary payer (vs Medicare) |
| Medicaid |
1.03 (0.99–1.08) |
0.12 |
| Private insurance |
1.02 (0.99–1.06) |
0.22 |
| Self-pay |
1.14 (1.06–1.22) |
<0.01 |
| No charge |
0.82 (0.63–1.07) |
0.14 |
| Other |
1.23 (1.16–1.31) |
<0.01 |
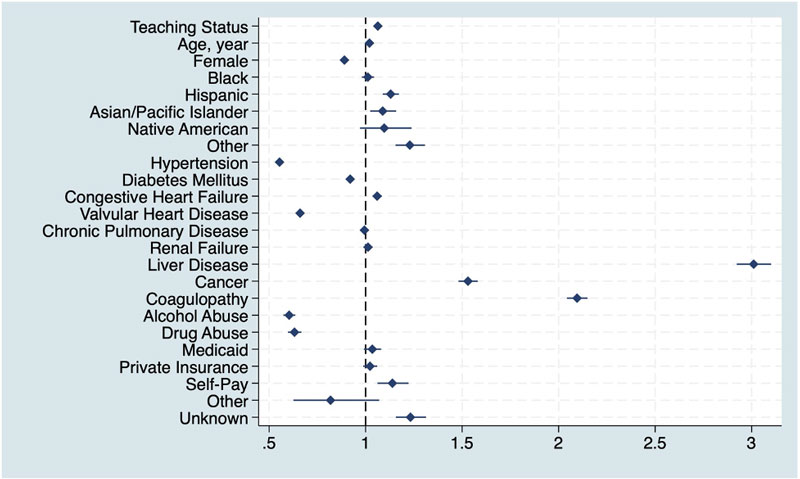
Figure 2 Adjusted odds ratios for predictors of in-hospital mortality in patients hospitalized with T2MI.
DISCUSSION
Type 2 myocardial infarction is an emerging myocardial infarction subtype that is caused by various systemic diseases that result in a demand and supply mismatch without significant coronary obstruction.4 Generally, patients with T2MI experience higher mortality and longer hospital stays compared to those with T1MI.5–7 This condition currently lacks established guidelines for diagnosis, risk stratification, and treatment.1 This gap could contribute to disparities in management and outcomes across different healthcare settings. Patients treated at teaching hospitals generally have better access to resources, which often results in improved outcomes.2
We found that the majority of patients with T2MI were admitted to urban teaching hospitals, comprising over three-quarters of the total T2MI cohort. Several factors may contribute to this distribution. First, there may be a falsely higher rate of T2MI diagnosis in urban teaching hospitals due to increased awareness and recognition among trainees and academic providers. Second, T2MI may be underdiagnosed in rural hospital settings, potentially due to limited access to advanced diagnostic modalities, such as imaging, which can help detect subtle wall motion abnormalities. A study by McCarthy et al. reported a misclassification rate of myocardial injury to T2MI of up to 41.9% at an academic hospital,8 where hospitalist services can sometimes misdiagnose T2MI as non-ST elevation myocardial infarction compared to cardiologists, as reported by Saleh et al.9
A notably low rate of PCI was observed in this T2MI cohort, with the highest rate reported among patients treated at urban teaching hospitals at only 1.5%. This low utilization raises concerns about the potential presence of undiagnosed underlying coronary artery disease, particularly given the high prevalence of comorbidities in this population that are commonly associated with atherosclerotic disease. These findings align with previous reports suggesting that invasive strategies and preventive pharmacotherapies may be underutilized in patients diagnosed with T2MI.10,11
We report a significantly higher mortality rate in urban teaching hospitals in T2MI patients compared to rural and urban non-teaching hospitals, with a longer duration of hospital stay and increased THC in the urban teaching hospitals. This finding contrasts with previous studies that have demonstrated significantly lower mortality rates related to surgical procedures, the management of complex patients, and cardiac arrest outcomes in urban teaching hospitals.12–14 This may be attributable to the lack of established evidence for diagnosis and treatment, which could contribute to undertreatment in this population.
After adjustment for potential confounders, treatment at urban teaching hospitals remained independently associated with increased odds of in-hospital mortality compared to other hospital types. Additional factors associated with higher mortality included advanced age, Hispanic and Asian race, and comorbidities such as liver disease, cancer, coagulopathy, and congestive heart failure. To date, disparities in healthcare delivery persist, with Hispanic and Asian populations often experiencing unequal treatment, potentially due to factors such as language barriers, insurance challenges, and immigration or documentation status.15,16 These factors may also complicate the treatment of the underlying illnesses associated with T2MI that result in increased morbidity and mortality. These findings underscore the need for the development of standardized guidelines for the diagnosis, risk stratification, and management of T2MI to improve outcomes and mitigate the risk of mortality, increased length of stay, and increased hospital charges.
LIMITATION
This study has several limitations. First, it is constrained by the administrative nature of the NIS. It is subject to coding errors or misclassification bias. Second, the diagnoses of T2MI were based on ICD-10-CM coding, which may not be accurate, as reported in a previous study. Third, the NIS lacks detailed clinical information and disease severity data that may impact clinical outcomes in this specific patient group. Last, the NIS captures hospitalizations rather than individual patients, which introduces the possibility that some individuals may have been counted more than once if they were admitted multiple times during the study period.
CONCLUSION
Our findings indicate higher mortality among T2MI patients treated at urban teaching hospitals, with urban teaching hospital status emerging as an independent predictor of in-hospital mortality. Establishing standardized guidelines for diagnosis, risk stratification, and treatment may help mitigate these risks and improve outcomes in these patients.
REFERENCES
- Sandoval Y, Jaffe AS. Type 2 Myocardial Infarction. JACC. 2019;73(14):1846–60. DOI: 10.1016/j.jacc.2019.02.018.
- Burke LG, Frakt AB, Khullar D, et al. Association between teaching status and mortality in US hospitals. Jama. 2017;317(20):2105–13. (In eng). DOI: 10.1001/jama.2017.5702.
- Zafar SN, Shah AA, Hashmi ZG, et al. Outcomes after emergency general surgery at teaching versus nonteaching hospitals. Journal of Trauma and Acute Care Surgery. 2015;78(1):69–77. DOI: 10.1097/ta.0000000000000493.
- Merlo AC, Bona RD, Ameri P, et al. Type 2 myocardial infarction: a diagnostic and therapeutic challenge in contemporary cardiology. Intern Emerg Med. 2022;17(2):317–24. (In eng). DOI: 10.1007/s11739-021-02920-8.
- Jaiswal V, Ang SP, Ishak A, et al. Comparison of outcome among type 2 vs type 1 myocardial infarction: a systematic review and meta-analysis. J Investig Med. 2023;71(3):223–34. DOI: 10.1177/10815589221140589.
- DeFilippis AP, Chapman AR, Mills NL, et al. Assessment and treatment of patients with type 2 myocardial infarction and acute nonischemic myocardial injury. Circulation. 2019;140(20):1661–78. DOI: 10.1161/CIRCULATIONAHA.119.040631.
- Raphael CE, Roger VL, Sandoval Y, et al. Incidence, trends, and outcomes of type 2 myocardial infarction in a community cohort. Circulation. 2020;141(6):454–63. DOI: 10.1161/CIRCULATIONAHA.119.043100.
- McCarthy C, Murphy S, Cohen JA, et al. Misclassification of myocardial injury as myocardial infarction: implications for assessing outcomes in value-based programs. JAMA Cardiology. 2019;4(5):460–4. DOI: 10.1001/jamacardio.2019.0716.
- Saleh MA, Ambrose JA, Poosti K, et al. Misdiagnosis of type II myocardial infarction. J Am Coll Cardiol. 2019;74(13):1732–3. (In eng). DOI: 10.1016/j.jacc.2019.07.052.
- Yao H, Zeller M, N’Guetta R, et al. Coronary artery disease: a key issue in type 2 myocardial infarction: systematic review and recent findings. J Clin Med. 2023;12(19) (In eng). DOI: 10.3390/jcm12196412.
- Baig MFA. Analysis of the weekend effect on mortality, diagnostic coronary angiography, and percutaneous coronary intervention in acute myocardial infarction across rural US hospitals. Cureus. 2024;16(2):e53751. DOI: 10.7759/cureus.53751.
- Czarnecki A, Qiu F, Koh M, et al. Association between hospital teaching status and outcomes after out-of-hospital cardiac arrest. Circulation: Cardiovascular Quality and Outcomes. 2019;12(12):e005349. DOI: 10.1161/CIRCOUTCOMES.118.005349.
- Hyder O, Sachs T, Ejaz A, et al. Impact of hospital teaching status on length of stay and mortality among patients undergoing complex hepatopancreaticobiliary surgery in the USA. Journal of Gastrointestinal Surgery. 2013;17(12):2114–22. DOI: 10.1007/s11605-013-2349-4.
- Ayanian JZ, Weissman JS. Teaching hospitals and quality of care: a review of the literature. Milbank Q. 2002;80(3):569–93, v. (In eng). DOI: 10.1111/1468-0009.00023.
- Cabral J, Cuevas AG. Health inequities among Latinos/Hispanics: documentation status as a determinant of health. J Racial Ethn Health Disparities. 2020;7(5):874–9. (In eng). DOI: 10.1007/s40615-020-00710-0.
- Lu FQ, Flores MW, Carson NJ, et al. Trends and disparities in mental health use among asian american sub-groups, 2013–2019. J Racial Ethn Health Disparities. 2024 (In eng). DOI: 10.1007/s40615-024-02177-9.
Article citation: Yanpiset P, Puchongmart C, Cruz D, Castillo-Rodriguez C, Sena J. Wonghanchai S, Shotelersuk V. The association between hospital teaching status and in-hospital outcomes among patients with type 2 myocardial infarction in the United States. The Southwest Journal of Medicine. 2026;14(59):1–7
From: Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, TX (PY, CP, DC, CC-R, JS, VS) Department of Family Medicine, Chakri Narubodindra Medical Institute, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Samut Prakan, Thailand
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.