Abstract
Ventricular arrhythmias and in-hospital outcomes in non-elective coronary artery bypass graft in type 1 myocardial infarction: An analysis of the national inpatient sample
Chanokporn Puchongmart MD, Varote Shotelersuk MD, Ben Thiravetyan MD, Panat Yanpiset MD, Thanaboon Yinadsawaphan MD, Narathorn Kulthamrongsri MD, Natnicha Leelaviwat MD, Zhaunn Sly MD
Corresponding author: Ben Thiravetyan
Contact Information: Ben.Thiravetyan@ttuhsc.edu
DOI: 10.12746/swjm.v14i60.1629
ABSTRACT
Background: Malignant ventricular arrhythmias (VAs) are a serious complication of type 1 myocardial infarction (T1MI), yet their burden and impact on outcomes in patients undergoing urgent coronary artery bypass grafting (CABG) are not well established.
Objectives: We aim to identify the incidence and the prognostic impact of malignant VAs in patients undergoing non-elective CABG for T1MI.
Methods: A retrospective cohort study using the National Inpatient Sample from 2016 to 2022 was conducted by identifying all adult patients with T1MI who underwent non-elective CABG. Survey-weighted analyses were performed to compare baseline characteristics and outcomes between VAs and non-VAs groups. Multivariable logistic regression was used to evaluate the independent association between VAs and in-hospital mortality.
Results: Among 388,310 weighted hospitalizations for T1MI undergoing CABG, 10.0% had malignant VAs. Patients with VAs were younger (65.6 vs. 65.4 years, p < 0.01), less likely to be female (21.7% vs. 26.8%, p < 0.01), and had higher rates of comorbid conditions. The presence of VAs was associated with higher in-hospital mortality (11.2% vs. 2.7%), longer hospital stay (12 vs. 8 days), and increased incidence of acute kidney injury (40.9% vs. 27.8%, p < 0.01). After adjustment, VAs remained independently associated with increased odds of in-hospital mortality (aOR 2.90, 95% CI 2.62-3.21).
Conclusions: VAs occur around 10% in patients undergoing CABG for T1MI and are strongly associated with an increase in in-hospital mortality. These findings underscore the importance of perioperative monitoring and management of VAs in this high-risk population.
Keywords: Ventricular tachycardia, ventricular fibrillation, myocardial infarction, coronary artery bypass graft
INTRODUCTION
Type 1 myocardial infarction (T1MI) remains the leading cause of death in the United States.1 It is characterized by acute atherothrombotic coronary artery occlusion by the Fourth Universal Definition of Acute Myocardial Infarction.2,3 The most common T1MI subtypes include acute coronary syndrome (ACS), such as ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI), which typically require revascularization therapy as part of their treatment.4 Coronary artery bypass grafting (CABG) is one of the well-established revascularization strategies that has been shown to improve survival and reduce major adverse cardiovascular events (MACE).5 In the context of T1MI, non-elective CABG can be performed in selected situations, such as failed or incomplete percutaneous coronary intervention (PCI), patients with high anatomical complexity, or mechanical complications of infarction.6
Ventricular arrhythmias (VAs) are among the most common arrhythmias following ischemic injury. VAs include conditions such as accelerated idiopathic ventricular rhythm, premature ventricular contractions, ventricular tachycardia (VT), and ventricular fibrillation (VF). Among these, the malignant VAs, such as VT and VF, were found to be linked to unfavorable in-hospital outcomes, such as increased in-hospital mortality, cardiogenic shock, heart failure, and acute kidney injury (AKI).7-9 Their pathophysiology often involves reentrant circuits that develop around ischemic or infarcted myocardium, leading to their occurrence during or after an acute myocardial infarction. Although the VAs in the context of coronary artery diseases and among patients undergoing elective CABG have been well studied,10-12 there is limited study on the burden and clinical impact of life-threatening VAs in patients undergoing non-elective CABG, specifically for patients hospitalized with T1MI. Given the substantial physiologic stress of surgery and the myocardial substrate associated with acute infarction, these patients may be more prone to develop VAs, potentially resulting in unfavorable in-hospital outcomes. Understanding the prevalence and prognostic significance of VAs in this context is crucial for evaluating perioperative risk and developing effective management strategies.
This study aimed to investigate the incidence and in-hospital outcomes of malignant VAs in patients with T1MI undergoing non-elective CABG, and to evaluate the association between malignant VAs and in-hospital mortality.
METHOD
We conducted a retrospective cohort study using the National Inpatient Sample (NIS) from 2016 to 2022. The NIS, part of the Healthcare Cost and Utilization Project (HCUP), is the largest publicly available all-payer inpatient database in the United States, providing a 20% stratified sample of discharges from U.S. community hospitals.
We included all adult patients (aged ≥ 18 years) who were hospitalized with a principal or secondary diagnosis of T1MI, identified using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis code I21.01, ST elevation (STEMI) myocardial infarction involving the left main coronary artery, code I21.02, ST elevation (STEMI) myocardial infarction involving left anterior descending coronary artery, code I21.09, ST elevation (STEMI) myocardial infarction involving other coronary artery of anterior wall, code I21.11, ST elevation (STEMI) myocardial infarction involving the right coronary artery, code I21.19, ST elevation (STEMI) myocardial infarction involving other coronary artery of inferior wall, I21.21, ST elevation (STEMI) myocardial infarction involving left circumflex coronary artery, I21.29, ST elevation (STEMI) myocardial infarction involving other sites, I21.3, Acute transmural myocardial infarction of unspecified site and I21.4, Non-ST elevation (NSTEMI) myocardial infarction. CABG procedures were identified using the ICD-10-CM diagnostic codes and Procedure Coding System procedure codes. Patients with missing data for key variables, e.g., age, sex, mortality, and race, were excluded.
The primary exposure was a diagnosis of malignant VAs, defined as the presence of ICD-10-CM codes I472, ventricular tachycardia, I4901, ventricular fibrillation, and I4902, ventricular flutter in any diagnosis field. Covariates, including age, sex, race, comorbidity burden, and percutaneous coronary intervention, were collected. Comorbidities were measured using individual Elixhauser comorbidity flags defined by HCUP software. Patients with heart failure were stratified by ejection fraction into groups with either reduced or preserved ejection fraction.
OUTCOMES
The primary outcome was the incidence of malignant VAs among patients hospitalized with non-elective CABG following T1MI. Secondary outcomes included in-hospital mortality, length of stay (LOS), and AKI.
STATISTICAL ANALYSIS
We applied survey weights, stratification, and clustering to all analyses to generate national estimates in accordance with HCUP guidelines. Descriptive statistics were used to summarize patients’ baseline characteristics. Continuous variables were reported as means ± standard deviations or medians with interquartile ranges as appropriate. Categorical variables were summarized as weighted percentages. Characteristics between patients with and without VAs were compared using design-based F tests from a survey-adjusted chi-square test. Continuous variables were reported as means with standard deviations or medians with interquartile ranges and compared using survey-weighted linear regression. Multivariable logistic regression was used to estimate the adjusted odds ratio (aOR) of in-hospital mortality associated with VAs. Confidence intervals and p-values <0.05 were considered statistically significant. All analyses were performed using Stata version 18.0 (StataCorp, College Station, TX).
RESULTS
From 2016 to 2022, a total of 388,310 patients were included in this analysis. Of these, 10.0% developed VAs. Baseline characteristics are summarized in Table 1. Patients who developed VAs were slightly older (65.6 ± 0.1 vs. 65.4 ± 0.0 years, p < 0.01) and less likely to be female (21.7% vs. 26.8%, p < 0.01). Significant racial differences were observed between the groups; however, most patients in both cohorts were White (76.3% in VAs and 74.4% in the non-VAs group). Most comorbidities differed significantly, except for cancer and drug abuse. Hypertension, diabetes, heart failure, obesity, chronic liver disease, and valvular heart disease were the most prevalent comorbid conditions, with notable differences between the VAs and non-VAs groups: hypertension (83.6% vs. 87.5%), diabetes (44.0% vs. 51.1%), heart failure (50.7% vs. 34.3%), obesity (26.3% vs. 30.3%), chronic liver disease (25.1% vs. 23.9%), and valvular heart disease (23.3% vs. 19.6%). Among patients with heart failure, those in the VAs group were more likely to have heart failure with reduced ejection fraction (HFrEF) (44.1% vs. 26.7%, p < 0.01) and slightly less likely to have heart failure with preserved ejection fraction (HFpEF) (6.6% vs. 7.6%, p < 0.01). Regarding the underlying cause of T1MI, STEMI was more common in patients with VAs (27.9% vs. 14.5%, p < 0.01), whereas NSTEMI was less frequent (72.8% vs. 85.8%, p < 0.01). Finally, patients with VAs were significantly more likely to undergo PCI (12.2% vs. 5.8%, p < 0.01).
Table 1. Baseline Characteristics of T1MI Patients who Underwent CABG with and Without Malignant VAs
| Characteristics |
Malignant VAs (N = 38,920) |
No Malignant VAs (N = 349,390) |
p-value |
| Incidence, % |
10.0 |
90.0 |
|
| Age, year |
65.6 ± 0.1 |
65.4 ± 0.0 |
|
| Female, % |
21.7 |
26.8 |
<0.01 |
| Race, % |
<0.01 |
| White |
76.3 |
74.4 |
|
| Black |
8.8 |
8.3 |
|
| Hispanic |
7.7 |
9.8 |
|
| Asian or Pacific islander |
3.5 |
3.7 |
|
| Native American |
0.6 |
0.7 |
|
| Others |
3.1 |
3.2 |
|
| Comorbidities, % |
| Hypertension |
83.6 |
87.5 |
<0.01 |
| Diabetes Mellitus |
44.0 |
51.1 |
<0.01 |
| Heart Failure |
|
|
|
| HFrEF |
44.1 |
26.7 |
<0.01 |
| HEpEF |
6.6 |
7.6 |
<0.01 |
| Chronic Kidney Disease |
25.1 |
23.9 |
0.02 |
| Valvular Heart Disease |
23.3 |
19.6 |
<0.01 |
| Liver Disease |
10.9 |
4.8 |
<0.01 |
| Obesity |
26.3 |
30.3 |
<0.01 |
| Cancer |
1.9 |
1.8 |
0.37 |
| Drug Abuse |
4.6 |
4.2 |
0.09 |
| Alcohol Abuse |
5.1 |
4.5 |
0.02 |
| Type of Myocardial Infarction, % |
<0.01 |
| STEMI |
27.9 |
14.5 |
<0.01 |
| NSTEMI |
72.8 |
85.8 |
<0.01 |
| Cardiogenic Shock, % |
28.6 |
11.4 |
<0.01 |
| Percutaneous Coronary Intervention, % |
12.2 |
5.8 |
<0.01 |
In the unadjusted analysis, patients with VAs experienced significantly unfavorable clinical outcomes, as summarized in Table 2. In-hospital mortality was notably higher in the VAs group (11.2% vs. 2.7%, p < 0.01), along with a longer LOS (12 vs. 8 days, p < 0.01) and a greater incidence of AKI (40.9% vs. 27.8%, p < 0.01).
Table 2. Unadjusted Outcomes Among Patients with and Without Malignant VAs
| Outcomes |
Malignant VAs (N = 38,920) |
No Malignant VAs (N = 349,390) |
p-value |
| In-hospital Mortality, % |
11.2 |
2.7 |
<0.01 |
| LOS, (IQR) |
8 (10-14) |
12 (9-18) |
<0.01 |
| Acute Kidney Injury, % |
40.9 |
27.8 |
<0.01 |
Multivariable logistic regression analysis for in-hospital mortality was demonstrated in Table 3 and Figure 1. The presence of VAs was independently associated with higher odds of in-hospital mortality (aOR 2.90, 95% CI 2.62-3.21). Older age was also a significant predictor (aOR 1.04, 95% CI 1.04-1.05). Other independent factors associated with higher mortality included female sex (aOR 1.76, 95% CI 1.61-1.92), Black race (aOR 1.26, 95% CI 1.08-1.45), cardiogenic shock (aOR 3.63, 95% CI 3.40-3.87), liver disease (aOR 6.17, 95% CI 5.67-6.72), and chronic kidney disease (aOR 1.68, 95% CI 1.56-1.81). Additionally, STEMI was also associated with increased odds of mortality (aOR 1.94, 95% CI 1.18-3.17), whereas NSTEMI did not show statistical significance between the two groups (aOR 1.28, 95% CI 0.78-2.10).
Table 3. Adjusted In-hospital Mortality Associated with and Without Malignant VAs
| Predictors |
In-hospital Mortality (aOR, 95% CI) |
p-value |
| Malignant VAs |
2.90 (2.62-3.21) |
<0.01 |
| Age, year |
1.04 (1.04-1.05) |
<0.01 |
| Female |
1.76 (1.61-1.92) |
<0.01 |
| Race |
| Black |
1.26 (1.08-1.45) |
<0.01 |
| Hispanic |
0.98 (0.84-1.13) |
0.75 |
| Asian or Pacific islander |
1.06 (0.86-1.31) |
0.56 |
| Native American |
1.37 (0.88-2.11) |
0.16 |
| Others |
1.13 (0.90-1.42) |
0.29 |
| Comorbidities |
| Hypertension |
0.69 (0.61-0.77) |
<0.01 |
| Diabetes Mellitus |
0.87 (0.80-0.95) |
<0.01 |
| Heart Failure |
|
<0.01 |
| HFrEF |
1.33 (1.20-1.47) |
<0.01 |
| HEpEF |
1.36 (1.17-1.58) |
<0.01 |
| Chronic Kidney Disease |
1.68 (1.53-1.84) |
<0.01 |
| Valvular Heart Disease |
1.22 (1.11-1.35) |
<0.01 |
| Liver Disease |
6.17 (5.56-6.86) |
<0.01 |
| Obesity |
0.82 (0.74-0.91) |
<0.01 |
| Alcohol Abuse |
0.70 (0.55-0.89) |
<0.01 |
| Type of Myocardial Infarction, % |
| STEMI |
1.94 (1.18-3.17) |
<0.01 |
| NSTEMI |
1.28 (0.78-2.10) |
0.32 |
| Cardiogenic Shock, % |
3.63 (3.29-4.00) |
<0.01 |
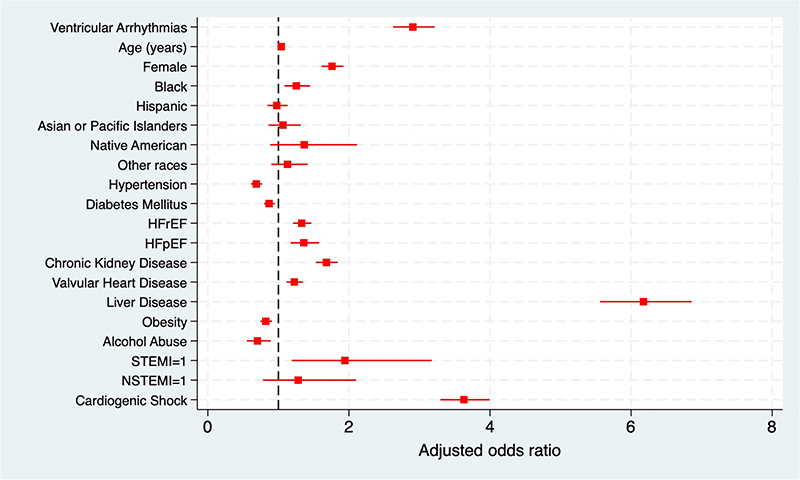
Figure 1. Adjusted odds ratio for in-hospital mortality in T1MI patients undergoing urgent CABG.
DISCUSSIONS
Ventricular arrhythmias are common in patients with ischemic myocardial injury, particularly among those with T1MI.13-18 The development of VAs in patients with T1MI undergoing non-elective CABG is likely attributable to the following mechanisms. First, the post-ischemic myocardium in T1MI is inherently more prone to electrical instability, thereby lowering the threshold for arrhythmia initiation.19 Second, the rapid reperfusion of ischemic myocardium during CABG could elicit reperfusion injury that provokes arrhythmias.20 Third, surgical manipulation and the associated inflammatory response heighten sympathetic activity and reduce vagal tone, creating a proarrhythmic autonomic imbalance.21 Fourth, the frequent use of inotropic agents during cardiac surgery can have direct proarrhythmic effects, further amplifying the risk.22 Fifth, the perioperative electrolytes disturbances could impair myocyte electrophysiologic properties and enhance myocyte automaticity which could provoke arrhythmias.23 The pathophysiology of ventricular arrhythmias in T1MI patients undergoing urgent CABG is illustrated in Figure 2.
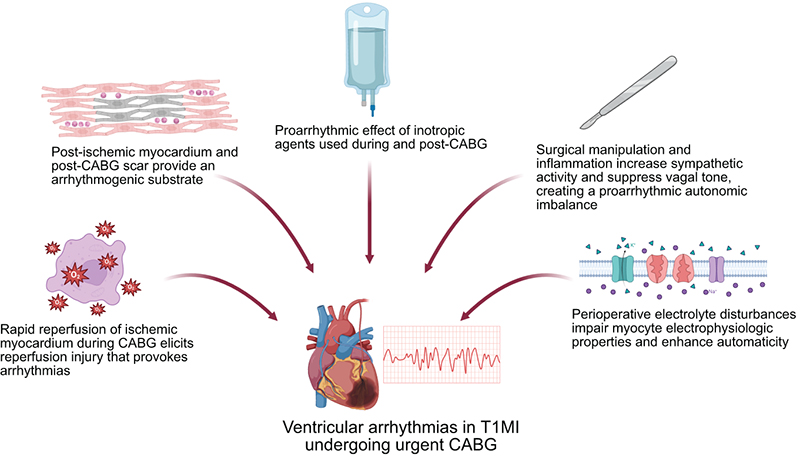
Figure 2. Pathophysiology of ventricular arrhythmias in T1MI patients undergoing urgent CABG.
Abbreviations: CABG = coronary artery bypass graft; T2MI = type 1 myocardial infarction
Created in BioRender. Thiravetyan, B. (2026) https://BioRender.com/ur7p48q
This study represents the first nationally representative cohort of patients with T1MI undergoing non-elective CABG. In this analysis, we observed a 10% incidence of malignant VAs in this high-risk population. The incidence of life-threatening VAs has been reported to be high among patients presenting with STEMI (4-9%), lower rates in those with NSTEMI (1.5%-4.6%),13-18 and relatively rare in patients without ACS who undergo elective CABG (0-3.1%).12,24 A recent study from Mouws et al. demonstrated an exceptionally high prevalence of non-significant premature ventricular contractions—up to 100% in non-elective CABG patients; however, none of these patients developed sustained VT or VF during the early postoperative period.12 This discrepancy may highlight differences in the underlying myocardial substrate or perioperative stress, as previously discussed. Additional proarrhythmic factors were also observed to be more prevalent among patients who developed malignant VAs in our study, including HFrEF, STEMI, cardiogenic shock, liver disease, and PCI, highlighting a greater baseline burden in this group.7,14,25
The in-hospital mortality rate among patients with malignant VAs was more than four times higher than in those without VAs (11.2% vs. 2.7%). Moreover, after adjusting for other clinical factors, the presence of malignant VAs remained independently associated with a 2.9-fold increase in the odds of in-hospital mortality in this population. These findings are consistent with, and notably stronger than, those reported by Wu et al., who observed a 1.9-fold increase in the risk of in-hospital MACE and cardiac death associated with malignant VAs in patients with STEMI undergoing PCI, which reflects the greater mortality risk among patients requiring CABG compared to those managed with PCI.7
In addition to mortality, the VAs group experienced longer duration of hospital stay and higher rates of AKI (40.9% vs. 27.8%), indicating a more complex hospital course and likely greater exposure to hemodynamic instability or nephrotoxic exposure.
Our study demonstrated a similar trend to that reported by Abbott et al., who found that STEMI was associated with a 4.1-fold increased risk of mortality in patients revascularized with PCI alone. However, we observed a lower magnitude of effect, with STEMI linked to a 1.94-fold higher odds of in-hospital mortality among patients undergoing non-elective CABG, while NSTEMI was not significantly associated with an increased mortality risk.26
Several other predictors of in-hospital mortality were also identified. Patients with liver disease had 6.2 times higher odds of in-hospital mortality, while those who developed cardiogenic shock had nearly fourfold higher odds. Chronic kidney disease was likewise associated with increased risk, with approximately 1.7 times higher odds of in-hospital mortality. Additionally, female sex and Black race were independently linked to higher mortality, aligning with previous studies that have documented disparities in cardiac surgical outcomes.27,28 Whether these differences are driven by underlying biological factors, delays in access to care, or broader inequities within the healthcare system remains unclear and warrants further investigation.
These findings highlight the need for malignant VAs’ risk stratification in T1MI patients undergoing non-elective CABG. Enhanced monitoring and preventive measures in the selected population might improve outcomes. Additionally, integrating VA occurrence into risk models could potentially enhance prognostic precision and guide postoperative care.
LIMITATIONS
This study has several limitations. First, it is constrained by the administrative nature of the NIS database, making it susceptible to coding errors and misclassification bias. Second, the identification of T1MI and malignant VAs was based on ICD-10-CM codes, which limits the ability to determine causal relationships between the incidence and prevalence of VAs among patients with T1MI, as some individuals may have had a prior diagnosis of VT or VF before hospitalization or cardiac surgery. Third, the NIS lacks detailed clinical data, including information on the severity of VAs, inotropic support during hospitalization, the degree of left ventricular dysfunction, and electrolyte disturbances, all of which could influence outcomes in this patient population. Fourth, because the NIS captures hospitalizations rather than individual patients, there is a possibility that some patients were included more than once if they had multiple admissions during the study period. Finally, due to the observational design of this study, a causal relationship between the presence of VAs and an increase in in-hospital mortality cannot be established.
CONCLUSION
The incidence of VT and VF in patients with T1MI undergoing non-elective CABG was 10%. These arrhythmias were independently associated with a 2.9-fold increase in the odds of in-hospital mortality.
REFERENCES
- Mortality in the United States, 2023. National Vital Statistics System.
- Khan MA, Hashim MJ, Mustafa H, et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus. 2020;12(7):e9349. DOI: 10.7759/cureus.9349.
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618-51. DOI: 10.1161/CIR.0000000
000000617.
- Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151(13):e771-862. DOI: 10.1161/CIR.0000000000001309.
- Head SJ, Kieser TM, Falk V, et al. Coronary artery bypass grafting: Part 1-the evolution over the first 50 years. Eur Heart J. 2013;34(37):2862-72. DOI: 10.1093/eurheartj/eht330.
- In: Watson TJ, Ong PJL, Tcheng JE, eds. Primary Angioplasty: A Practical Guide. Singapore 2018.
- Wu X, Wu M, Huang H, et al. Incidence, predictors, and prognostic impact of reperfusion-related ventricular arrhythmias in STEMI patients undergoing primary percutaneous coronary intervention. BMC Cardiovasc Disord. 2025;25(1):494. DOI: 10.1186/s12872-025-04953-9.
- Gorenek B, Blomström Lundqvist C, Brugada Terradellas J, et al. Cardiac arrhythmias in acute coronary syndromes: position paper from the joint EHRA, ACCA, and EAPCI task force. EP Europace. 2014;16(11):1655-73. DOI: 10.1093/europace/euu208.
- Kanabar K, Sharma YP, Krishnappa D, et al. A study of the predictive role of multiple variables for the incidence of acute kidney injury and its outcomes in Indian patients with ST-elevation myocardial infarction and cardiogenic shock. The Egyptian Heart Journal. 2024;76(1):123. DOI: 10.1186/s43044-024-00557-4.
- Frampton J, Ortengren AR, Zeitler EP. Arrhythmias After Acute Myocardial Infarction. Yale J Biol Med. 2023;96(1):83-94. DOI: 10.59249/LSWK8578.
- Rubin DA, Nieminski KE, Monteferrante JC, et al. Ventricular arrhythmias after coronary artery bypass graft surgery: incidence, risk factors and long-term prognosis. J Am Coll Cardiol. 1985;6(2):307-10. (In eng). DOI: 10.1016/s0735-1097(85)80165-0.
- Mouws EMJP, Yaksh A, Knops P, et al. Early ventricular tachyarrhythmias after coronary artery bypass grafting surgery: Is it a real burden? Journal of Cardiology. 2017;70(3):263-70. DOI: https://doi.org/10.1016/j.jjcc.2016.12.001.
- Mehta RH, Starr AZ, Lopes RD, et al. Incidence of and outcomes associated with ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention. JAMA. 2009;301(17):1779-89. DOI: 10.1001/jama.2009.600.
- Rymer JA, Wegermann ZK, Wang TY, et al. Ventricular Arrhythmias After Primary Percutaneous Coronary Intervention for STEMI. JAMA Netw Open. 2024;7(5):e2410288. DOI: 10.1001/jamanetworkopen.2024.10288.
- Mehta RH, Yu J, Piccini JP, et al. Prognostic significance of postprocedural sustained ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention (from the HORIZONS-AMI Trial). Am J Cardiol. 2012;109(6):805-12. DOI: 10.1016/j.amjcard.2011.10.043.
- Amin M, Kella D, Killu AM, et al. Sudden cardiac arrest and ventricular arrhythmias following first type I myocardial infarction in the contemporary era. J Cardiovasc Electrophysiol. 2019;30(12):2869-76. (In eng). DOI: 10.1111/jce.14218.
- Tran HV, Ash AS, Gore JM, et al. Twenty-five year trends (1986-2011) in hospital incidence and case-fatality rates of ventricular tachycardia and ventricular fibrillation complicating acute myocardial infarction. Am Heart J. 2019;208:1-10. (In eng). DOI: 10.1016/j.ahj.2018.10.007.
- Schnur A, Rav Acha M, Loutati R, et al. Incidence of Ventricular Fibrillation and Sustained Ventricular Tachycardia Complicating Non-ST Segment Elevation Myocardial Infarction. J Clin Med. 2024;13(8). (In eng). DOI: 10.3390/jcm13082286.
- Sattler SM, Skibsbye L, Linz D, et al. Ventricular Arrhythmias in First Acute Myocardial Infarction: Epidemiology, Mechanisms, and Interventions in Large Animal Models. Front Cardiovasc Med. 2019;6:158. (In eng). DOI: 10.3389/fcvm.2019.00158.
- Ayoub CM, Sfeir PM, Bou-Khalil P, et al. Prophylactic amiodarone versus lidocaine for prevention of reperfusion ventricular fibrillation after release of aortic cross-clamp. Eur J Anaesthesiol. 2009;26(12):1056-60. (In eng). DOI: 10.1097/EJA.0b013e32832f0dfb.
- Walsh SR, Tang T, Wijewardena C, et al. Postoperative arrhythmias in general surgical patients. Ann R Coll Surg Engl. 2007;89(2):91-5. (In eng). DOI: 10.1308/003588407x168253.
- Tisdale JE, Patel R, Webb CR, et al. Electrophysiologic and proarrhythmic effects of intravenous inotropic agents. Prog Cardiovasc Dis. 1995;38(2):167-80. (In eng). DOI: 10.1016/s0033-0620(05)80005-2.
- Peretto G, Durante A, Limite LR, et al. Postoperative arrhythmias after cardiac surgery: incidence, risk factors, and therapeutic management. Cardiol Res Pract. 2014;2014:615987. (In eng). DOI: 10.1155/2014/615987.
- Steinberg JS, Gaur A, Sciacca R, et al. New-Onset Sustained Ventricular Tachycardia After Cardiac Surgery. Circulation. 1999;99(7):903-8. DOI: 10.1161/01.CIR.99.7.903.
- Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2018;15(10):e190-252. DOI: 10.1016/j.hrthm.2017.10.035.
- Abbott JD, Ahmed HN, Vlachos HA, et al. Comparison of Outcome in Patients With ST-Elevation Versus Non-ST-Elevation Acute Myocardial Infarction Treated With Percutaneous Coronary Intervention (from the National Heart, Lung, and Blood Institute Dynamic Registry). The American Journal of Cardiology. 2007;100(2):190-5. DOI: https://doi.org/10.1016/j.amjcard.2007.02.083.
- Zea-Vera R, Asokan S, Shah RM, et al. Racial/ethnic differences persist in treatment choice and outcomes in isolated intervention for coronary artery disease. J Thorac Cardiovasc Surg. 2023;166(4):1087-96 e5. DOI: 10.1016/j.jtcvs.2022.01.034.
- Mehta LS, Beckie TM, DeVon HA, et al. Acute Myocardial Infarction in Women: A Scientific Statement From the American Heart Association. Circulation. 2016;133(9):916-47. DOI: 10.1161/CIR.0000000000000351.
Article citation: Puchongmart C, Shotelersuk V, Thiravetyan B, Yanpiset P, Yinadsawaphan T, Kulthamrongsri N, Leelaviwat N, Sly Z. Ventricular arrhythmias and in-hospital outcomes in non-elective coronary artery bypass graft in type 1 myocardial infarction: An analysis of the national inpatient sample. The Southwest Journal of Medicine. 2026;14(60):8-16
From: Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas (CP, VS, BT, NL, SZ) Department of Internal Medicine, John A Burns School of Medicine, Honolulu, HI (TY, NK)
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.