Abstract
A rare case of opportunistic Kluyvera bloodstream infection in a pediatric patient with supratentorial ependymoma
Moiz Ahmed Khan MBBS, Syeda Bushra Fatima BSc, MS, Summaya Zafar MBBS, Muhammad Rafay MBBS
Corresponding author: Moiz Ahmed Khan
Contact Information: Moiz_online@yahoo.com
DOI: 10.12746/swjm.v14i60.1645
ABSTRACT
A 2.5-year-old girl with a history of surgically resected supratentorial ependymoma WHO grade 3 developed a central line-associated bloodstream infection (CLABSI) during hospitalization for intensity-modulated radiation therapy (IMRT). The patient had a peripherally inserted central catheter (PICC) line placed for management and developed fever five days post-insertion. Blood cultures from both PICC line and peripheral vein grew Kluyvera species, a rare gram-negative opportunistic pathogen from the Enterobacteriaceae family. The organism was susceptible to several antibiotics including piperacillin-tazobactam, carbapenems and aminoglycosides. The infected PICC line was removed, and the patient received systemic antibiotic therapy with piperacillin-tazobactam. Clinical improvement was observed within three days, with complete recovery from the infection achieved after five days of treatment. This case highlights the potential for Kluyvera spp. to cause CLABSI in immunocompromised pediatric oncology patients. It underscores the importance of prompt recognition, appropriate antibiotic therapy, and heightened surveillance and infection prevention strategies in this vulnerable population.
Keywords: Kluyvera species, Central line-associated bloodstream infection, Pediatric oncology, Ependymoma, PICC line, Opportunistic pathogen
INTRODUCTION
Kluyvera species are gram-negative, facultatively anaerobic bacteria belonging to the Enterobacteriaceae family that were first described in 1936.1 These organisms are ubiquitous in the environment, particularly in water, soil, and sewage and have been identified as normal flora in the human digestive tract. While historically considered opportunistic pathogens with low virulence, Kluyvera spp. have emerged as causative agents of clinically significant infections, particularly in immunocompromised hosts.2
In the pediatric population, Kluyvera infections are rare but have been associated with a spectrum of clinical presentations ranging from urinary tract infections to life-threatening sepsis with multiorgan failure.2 The organism exhibits intrinsic resistance to ampicillin and first- and second-generation cephalosporins; however, typically remains susceptible to third-generation cephalosporins, aminoglycosides, fluoroquinolones and carbapenems.3,4
Central line-associated bloodstream infections (CLABSIs) represent a significant complication in pediatric oncology patients, with incidence rates of approximately 1.51 per 1000 central venous catheter-days.5 These infections not only necessitate antibiotic treatment but often require catheter removal and prolonged hospitalizations.5,6 Pediatric oncology patients are particularly susceptible to CLABSI due to their immunocompromised state, frequent neutropenia and prolonged need for central venous access.5,7
Supratentorial ependymomas constitute approximately 30% of all pediatric ependymomas and are characterized by distinct molecular and clinical features.8 WHO grade 3 (anaplastic) ependymomas are aggressive tumors with higher rates of recurrence and metastasis compared to lower-grade variants.8 The standard treatment approach involves maximal surgical resection followed by adjuvant radiation therapy, with intensity-modulated radiation therapy (IMRT) being increasingly utilized to minimize dose to normal brain tissue.8,9
Herein, we report a rare case of Kluyvera spp. CLABSI in a pediatric patient with supratentorial ependymoma undergoing adjuvant radiation therapy, highlighting the clinical significance of this opportunistic pathogen in immunocompromised pediatric patients.
CASE PRESENTATION
A 2.5-year-old female patient with a known history of supratentorial ependymoma and surgical excision, presented for intensity-modulated radiation therapy (IMRT) management. The patient had initially presented six months prior with vomiting and seizures, and imaging studies revealed a supratentorial space-occupying lesion. Pre-operative Magnetic Resonance Imaging (MRI) on February 18, 2025, demonstrated a lesion in the fronto-parietal region measuring 2.9 × 5.1 × 5.5 cm with anterior cystic components and slight midline shift. The patient underwent craniotomy with excisional biopsy, and histopathological examination confirmed high-grade supratentorial ependymoma WHO grade 3. Post-operative MRI on April 26, 2025, showed a residual lesion in the left parietal region measuring 3.4 × 3.4 × 3.3 cm with surrounding enhancement and cystic areas.
Due to the large residual lesion,which was not amenable to further surgical resection, the patient was referred for adjuvant IMRT. Physical examination revealed a well-oriented and alert child with right-sided motor weakness with power of 4/5 in both upper and lower limbs. The patient was admitted for further management and underwent insertion of a peripherally inserted central catheter (PICC) line for medication administration and supportive care.
Five days following PICC line insertion, the patient developed a fever of 102°F. Physical examination revealed stable vital signs with clear chest examination and soft abdomen. Two sets of blood cultures were obtained, one from the PICC line and one from a peripheral vein. Both sets of blood cultures became positive after 48 hours of incubation, with Gram stain revealing gram-negative rods (Figure 1). Subculture on chocolate agar, 5% sheep blood agar and MacConkey agar demonstrated growth of round, convex, yellow-colored, non-lactose fermenting and oxidase-negative colonies after 48 hours of aerobic incubation (Figure 2).
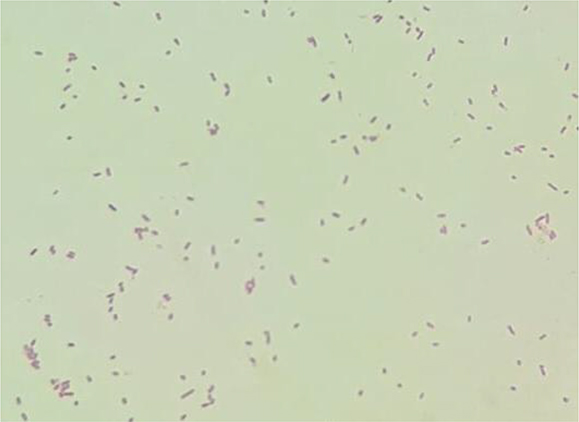
Figure 1. Gram stain morphology of Kluyvera species.
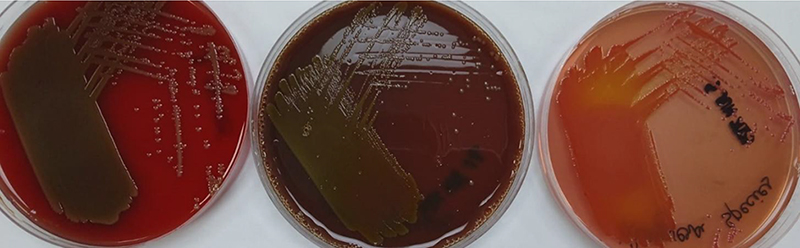
Figure 2. Colony morphology of Kluyvera species on Chocolate agar, 5% Sheep blood agar and MacConkey agar.
The organism was identified as a Kluyvera species using API® ID strips and APIWEB™ database. Antimicrobial susceptibility testing was performed using Kirby-Bauer disk diffusion method, with interpretation according to Clinical and Laboratory Standards Institute (CLSI) M100 guidelines.10 The isolate demonstrated sensitivity to amikacin, gentamicin, ceftriaxone, cefixime, ciprofloxacin, co-trimoxazole, piperacillin-tazobactam, imipenem and meropenem.
A diagnosis of CLABSI was established after ruling out other sources of bacteremia. The patient was initiated on intravenous piperacillin-tazobactam. The infected PICC line was removed and systemic antibiotic therapy was continued. Clinical improvement was noted within three days of treatment initiation, with resolution of fever and improvement in general condition. The patient achieved complete recovery from the infection after 5 days of treatment.
DISCUSSION
This case represents a rare occurrence of Kluyvera spp. causing CLABSI in a pediatric patient with supratentorial ependymoma. While Kluyvera infections have been reported in the pediatric population, they remain uncommon, particularly in the context of central line-associated infections.1,2 The clinical significance of this case lies in several important aspects.
Firstly, the patient population represents a particularly vulnerable group. Pediatric oncology patients, especially those with brain tumors undergoing active treatment, are at increased risk for healthcare-associated infections due to immunosuppression, frequent hospitalizations and need for invasive procedures.5,7 Furthermore, the identification of Kluyvera spp. in this case required careful microbiological evaluation. These organisms can be challenging to identify due to their phylogenetic similarity to other Enterobacteriaceae, including Enterobacter, Klebsiella and Citrobacter.11 Recent studies have highlighted potential misidentification by molecular diagnostic panels, emphasizing the importance of conventional culture methods and standardized antimicrobial susceptibility testing.11
The antimicrobial susceptibility profile demonstrated in this case is consistent with previously reported patterns for Kluyvera spp. The organism showed sensitivity to broad-spectrum antibiotics including piperacillin-tazobactam, carbapenems and aminoglycosides, while typically demonstrating intrinsic resistance to ampicillin and first-generation cephalosporins.3,4 This susceptibility pattern is crucial for clinicians managing Kluyvera infections, as an inappropriate initial antimicrobial therapy can lead to treatment failure and complications.
The clinical course in this case was favorable, with prompt clinical improvement following appropriate antimicrobial therapy and catheter removal. This outcome aligns with previous pediatric case series reporting good clinical responses to third-generation cephalosporins, aminoglycosides and beta-lactam/beta-lactamase inhibitor combinations.1,4
Risk factors for CLABSI in pediatric oncology patients include prolonged catheter duration, neutropenia, malnutrition and underlying malignancy.12 In this case, the patient had recently undergone neurosurgical procedures and was receiving treatment for a high-grade brain tumor, both factors that could contribute to immunosuppression and increased infection risk.7
The emergence of Kluyvera spp. as opportunistic pathogens in immunocompromised patients have important implications for infection prevention and antimicrobial stewardship. These organisms serve as reservoirs for extended-spectrum beta-lactamase (ESBL) genes, particularly CTX-M variants, which can be transferred to other Enterobacteriaceae.13 While the isolate in this case remained susceptible to multiple antimicrobials, clinicians should be aware of the potential for resistance development and the importance of appropriate antimicrobial selection. The successful management of this case highlights the importance of prompt recognition of CLABSI, appropriate microbiological evaluation and timely intervention with catheter removal and antimicrobial therapy.
CONCLUSION
We reported a rare case of Kluyvera species CLABSI in a pediatric patient with supratentorial ependymoma. The successful management of this infection demonstrates the importance of maintaining high clinical suspicion for opportunistic pathogens in immunocompromised pediatric oncology patients. Prompt recognition, appropriate microbiological evaluation and timely intervention with catheter removal and antimicrobial therapy are crucial for favorable outcomes.
REFERENCES
- Karadağ Öncel E, Özsürekci Y, Akyön Y, et al. Kluyvera ascorbata infections in children: a case series. Turk Pediatri Ars. 2015;50(2):123-8.
- Carter JE, Laurini JA, Mizell KN. Kluyvera infections in the pediatric population. Pediatr Infect Dis J. 2008;27(9):839-41.
- Stock I. Natural antimicrobial susceptibility patterns of Kluyvera ascorbata and Kluyvera cryocrescens strains and review of the clinical efficacy of antimicrobial agents used for the treatment of Kluyvera infections. J Chemother. 2005;17(2):143-60.
- Carter JE, Evans TN. Clinically significant Kluyvera infections: a report of seven cases. Am J Clin Pathol. 2005;123(3):334-8.
- van den Bosch CH, Kops AL, Loeffen YGT, et al. Central venous catheter-related bloodstream infections caused by Enterobacterales in pediatric oncology patients: catheter salvage or removal. Pediatr Infect Dis J. 2024;43(1):49-55.
- Walker LW, Visweswaran S, Nowalk AJ. Outcomes in pediatric central line-associated bloodstream infections treated with antimicrobial locks: a 14-year retrospective analysis. Pediatr Infect Dis J. 2023;42(6):473-8.
- Li L, Zheng Y, Deng W, et al. Central line-associated bloodstream infections in children: a systematic review and meta-analysis. Transl Pediatr. 2025;14(5):799-811.
- Jünger ST, Timmermann B, Pietsch T. Pediatric ependymoma: an overview of a complex disease. Childs Nerv Syst. 2021;37(8):2451-63.
- Landau E, Boop FA, Conklin HM, et al. Supratentorial ependymoma: disease control, complications, and functional outcomes after irradiation. Int J Radiat Oncol Biol Phys. 2013;85(4):e193-e199.
- Clinical & Laboratory Standards Institute M100 Ed35.
- Vatterrodt D, Lee J, Ho D, et al. Misidentification and misreporting of antibiotic resistance in Kluyvera bacteremia by blood culture molecular identification panels. Microbiol Spectr. 2024;12(6):e00542-24.
- Rabelo BS, de Alvarenga KAF, Miranda JWFB, et al. Risk factors for catheter-related infection in children with cancer: a systematic review and meta-analysis. Am J Infect Control. 2023;51(1):99-106.
- Yu K, Huang Z, Lan R, et al. Genomic characterization of opportunistic pathogen Kluyvera reveals a novel CTX-M subgroup. Microorganisms. 2023;11(12):2836.
Article citation: Khan M, Fatima S, Zafar S, Rafay M. A rare case of opportunistic Kluyvera bloodstream infection in a pediatric patient with supratentorial ependymoma. The Southwest Journal of Medicine. 2026;14(60):67–70
From: Department of Clinical Laboratory, Indus Hospital & Health Network, Karachi, Pakistan (MK, SF) Clinical Laboratory, Tabba Heart Institute, Karachi, Pakistan (MK) Pathology and Laboratory Medicine, Aga Khan University, Karachi, Pakistan (SZ) Neurosurgery, Liaquat National Hospital and Medical College, Karachi, Pakistan (MR)
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.