INTRODUCTION
Respiratory syncytial virus (RSV) is an important and often under-recognized cause of acute respiratory infection in adults, with the greatest clinical impact in older adults and in adults with chronic cardiopulmonary disease or other high-risk conditions. RSV infection occurred annually in community-dwelling adults aged 65 years or older and in high-risk adults with chronic heart or lung disease. In hospitalized adults, the clinical severity of RSV was comparable to that of influenza A with respect to intensive care use and mortality.1
Global and regional burden estimates in older adults underscore the public health relevance of RSV prevention strategies in adult populations. A systematic review and meta-analysis estimated that in 2015 there were approximately 336,000 RSV-associated acute respiratory infection hospitalizations and about 14,000 in-hospital deaths among older adults globally, while acknowledging limited data availability from many low- and middle-income settings.2 In high-income countries, pooled estimates suggest that RSV in adults aged 60 years and older translated in 2019 to approximately 5.2 million cases, 470,000 hospitalizations, and 33,000 in-hospital deaths.3 In the United States, a systematic review and meta-analysis estimated a pooled annual RSV-associated hospitalization incidence of 178 per 100,000 adults aged 65 years and older; after adjustment for under-detection, the estimated hospitalization rate increased to 267 per 100,000, and adults with chronic medical conditions were substantially more likely to be hospitalized for RSV, depending on the specific risk condition.4
Because severe RSV outcomes disproportionately affect older adults and medically vulnerable adults, multiple RSV vaccine platforms have advanced through adult clinical trials, including prefusion F protein subunit vaccines (RSVpreF) with and without adjuvant, a messenger RNA (mRNA)-based prefusion F vaccine, and investigational viral-vectored approaches. However, direct head-to-head comparisons are lacking, and an integrated synthesis of clinical trial vaccine efficacy, real-world vaccine effectiveness, durability across seasons, and post-licensure safety signals remains incompletely characterized. Therefore, we conducted this narrative review to summarize and compare the available evidence on RSV vaccine efficacy, effectiveness, and safety in adults, with emphasis on older adults and other high-risk populations.
METHOD
This narrative review summarizes evidence on RSV vaccine efficacy, real-world effectiveness, and safety in adults, with emphasis on healthy adults aged 18-59 years, older adults aged >60 years, and clinically vulnerable subgroups including immunocompromised patients. We searched PubMed and Embase and supplemented these searches by reviewing reference lists from pivotal clinical trials, real-world effectiveness studies, and meta-analyses. Search concepts included RSV or respiratory syncytial virus, vaccine, prefusion F or preF, efficacy, effectiveness, safety, adverse events, and product or platform terms relevant to adult vaccines and late-stage candidates, including RSVpreF or Abrysvo, RSV prefusion F protein 3 (RSVPreF3) or Arexvy, mRNA-1345 or mResvia, adenovirus serotype 26 RSV prefusion F vaccine (Ad26.RSV.preF), and Modified vaccinia Ankara-vectored multivalent RSV vaccine (MVA-BN-RSV).
We included randomized controlled trials, including controlled human challenge studies, multi-season follow-up analyses, subgroup analyses in adults with comorbidities, observational effectiveness studies such as test-negative designs and target trial emulations, and systematic reviews or meta-analyses reporting quantitative outcomes in adults. We excluded studies limited to pediatric populations, maternal immunization, or infant monoclonal antibody products unless adult-specific outcomes relevant to this review were reported.
Data were extracted by the reviewer using a structured approach aligned with the evidence tables. For each included study, we abstracted the vaccine platform and product, including manufacturer and trade name when available; population characteristics and key comorbidities; study design and setting; comparator; follow-up duration and RSV season or seasons; point estimates of vaccine efficacy and effectiveness with corresponding confidence intervals (CI) (Figure 1); and safety outcomes, including reactogenicity, adverse events, serious adverse events, and prespecified rare events such as Guillain-Barré syndrome (GBS) or immune thrombocytopenia (ITP) when available. The extracted data were summarized in Table 1 for clinical trial outcomes and in Table 2 for real-world outcomes. Findings were synthesized qualitatively, with attention to heterogeneity in study design, endpoint definitions, and seasonality that may limit cross-study comparisons.
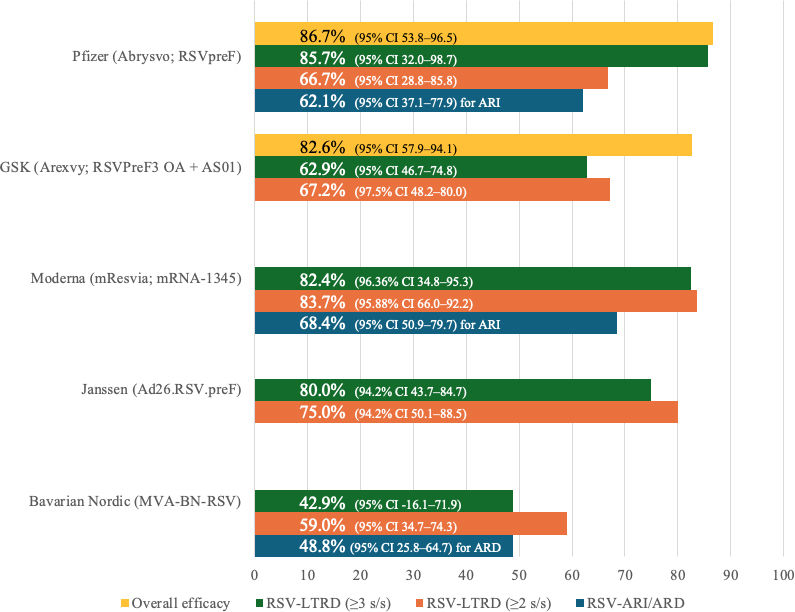
Figure 1. RSV vaccine efficacy.
Abbreviations: ARD, acute respiratory disease; ARI, acute respiratory infection; CI, confidence interval; LRTD, lower respiratory tract disease; RSV, respiratory syncytial virus; s/s, signs and/or symptoms.
RESULTS
CLINICAL TRIAL EFFICACY OF THE RSV VACCINE PLATFORM
UNADJUVANTED BIVALENT RSVPREF PROTEIN SUBUNIT VACCINE
Abrysvo (RSVpreF; Pfizer) is a stabilized prefusion F protein subunit vaccine containing antigens from both RSV-A and RSV-B. In a controlled human challenge study in adults aged 18-50 years, RSVpreF-based vaccination demonstrated vaccine efficacy 86.7% (95% CI, 53.8-96.5) vs placebo. Vaccinated participants had lower detectable viral ribonucleic acid (RNA); the median area under the curve of RSV viral load was 0 (interquartile range, 0.0-19.0) in the vaccine group vs 96.7 (interquartile range, 0.0-675.3) in the placebo group.5
In the phase 3 RENOIR trial among adults aged ≥60 years (including participants with stable chronic conditions), Abrysvo reduced RSV-associated lower respiratory tract disease (RSV-LRTD) during the first RSV season, with efficacy dependent on endpoint stringency. vaccine efficacy was 66.7% (95% CI, 28.8-85.8) against RSV-LRTD meeting a ≥2 signs/symptoms (s/s) threshold and 85.7% (95% CI, 32.0-98.7) against RSV-LRTD meeting a ≥3 s/s threshold; vaccine efficacy against RSV-associated acute respiratory infection (RSV-ARI) was 62.1% (95% CI, 37.1-77.9).6
A subsequent two-season analysis from RENOIR indicated persistence of protection over two RSV seasons for Abrysvo. Age-stratified vaccine efficacy point estimates were 81.6% (95% CI, 58.2-93.1) in adults aged 60-69 years, 72.7% (95% CI,−3.2-95.1) in adults aged 70-79 years, and 100% (95% CI,−9.1-100) in adults aged >80 years with ≥3 s/s. An overall vaccine efficacy estimate of 57.5% (95% CI, 35.8-72.4) was reported for RSV-LRTD using a ≥2 s/s definition.7
ADJUVANTED RSVPREF3 PROTEIN SUBUNIT VACCINE
Arexvy (RSVPreF3 + AS01; GSK) uses a recombinant preF antigen (RSVPreF3, based on RSV-A) combined with the AS01 adjuvant system. In a phase 3 randomized, placebo-controlled trial in adults aged ≥60 years, RSVPreF3 OA demonstrated high first-season efficacy against RSV-LRTD, with vaccine efficacy of 82.6% (95% CI, 57.9-94.1). Protection against severe RSV-LRTD was higher, with vaccine efficacy of 94.1% (95% CI, 62.4-99.9).8 Across a two-season follow-up, protection with Arexvy remained statistically significant. Still, it was attenuated in the second season: vaccine efficacy was 67.2% (97.5% CI, 48.2-80.0) against RSV-LRTD and 78.8% (95% CI, 52.5-92.0) against severe RSV-LRTD.9 In a subgroup analysis of participants with underlying medical conditions, vaccine efficacy remained robust, with vaccine efficacy 81.0% (95% CI, 58.9-92.3) in those with >1 condition and vaccine efficacy 88.0% (95% CI, 60.9-97.7) in those with >2 conditions.10
Over three RSV seasons, overall efficacy against RSV-LRTD with Arexvy declined over time but remained clinically meaningful: vaccine efficacy 62.9% (95% CI, 46.7-74.8) across three seasons. Strain-specific estimates were vaccine efficacy 69.8% (95% CI, 42.2-85.7) for RSV-A-related LRTD and 58.6% (95% CI, 35.9-74.1) for RSV-B-related LRTD, indicating cross-subtype protection despite an RSV-A-based antigen.11
MRNA VACCINE ENCODING RSV PREF (RSV-A PREF)
mResvia (mRNA-1345; Moderna) is an mRNA vaccine encoding a stabilized prefusion F glycoprotein (RSV subtype A) expressed in vivo after intramuscular administration. In a phase 2/3 randomized, placebo-controlled trial in adults aged ≥60 years (including participants with coexisting conditions), mRNA-1345 demonstrated high efficacy over 1 year: 83.7% (95.88% CI, 66.0-92.2) against RSV-LRTD (≥2 s/s) and 82.4% (96.36% CI, 34.8-95.3) against RSV-LRTD (≥3 s/s). Vaccine efficacy against RSV-ARI was 68.4% (95% CI, 50.9-79.7).12
ADENOVIRUS-VECTORED RSV PREF PLUS RSV PREF PROTEIN VACCINE
Janssen evaluated an investigational combination approach using a replication-incompetent Ad26-vectored RSV preF construct together with the RSV preF protein. In adults aged ≥65 years with coexisting conditions, the phase 2b CYPRESS trial demonstrated efficacy over the first RSV season: 80.0% (94.2% CI, 43.7-84.7) against RSV-LRTD meeting a ≥3 s/s threshold and 75.0% (94.2% CI, 50.1-88.5) against RSV-LRTD meeting a ≥2 s/s threshold.13
Multi-season follow-up of the Janssen investigational Ad26.RSV.preF/RSV preF protein vaccine indicated sustained protection beyond the first season, with efficacy of 76.1% (95% CI, 26.9-94.2) across seasons two and three and 78.7% (95% CI, 57.3-90.4) across three seasons combined.14 In a phase 3 study in Japan (cohort ≥60 years for efficacy), the trial was terminated early with few RSV events; point estimates were vaccine efficacy of 58.7% (95% CI, 245-100) for RSV-LRTD and 66.5% (95% CI, 717.68-99.36) for another RSV outcome as reported. Still, interpretation was limited due to premature termination and sparse endpoints.15
MODIFIED VACCINIA ANKARA-VECTORED MULTIVALENT RSV VACCINE
MVA-BN-RSV (Bavarian Nordic) is an investigational modified vaccinia Ankara-vectored multivalent RSV vaccine encoding multiple RSV antigens, including F, glycoproteins from both RSV subtypes (G[A] and G[B]), and internal proteins. In a human challenge trial in healthy adults aged 20-59 years, efficacy in preventing symptomatic infection in the challenge model ranged from 79.3% to 88.5%, accompanied by reductions in viral load and symptoms compared with placebo.16
In a phase 3 randomized trial in adults aged ≥60 years, efficacy with MVA-BN-RSV was more modest: 42.9% (95% CI, −16.1-71.9) against RSV-LRTD defined by ≥3 s/s, 59.0% (95% CI, 34.7-74.3) against RSV-LRTD defined by ≥2 s/s, and 48.8% (95% CI, 25.8-64.7) against acute respiratory disease.17
POOLED EFFICACY ACROSS VACCINE PRODUCTS
A systematic review and meta-analysis of randomized trials in older adults found that RSV vaccines reduced RSV-related LRTD (vaccine efficacy of 78.3% [95% CI, 65.6-86.3]) and RSV-related severe LRTD (vaccine efficacy of 86.5% [95% CI, 68.3-94.3]) and also reduced RSV-related ARI (vaccine efficacy of 68.0% [95% CI, 58.5-75.3]). This analysis reported no significant difference in the incidence of serious adverse events between the groups.18
REAL-WORLD VACCINE EFFECTIVENESS IN ADULTS AGED ≥60 YEARS
OVERALL EFFECTIVENESS IN TYPICAL ADULTS AGED ≥60 YEARS
Across US test-negative and emulated trial designs during the 2023-2024 season(s), real-world vaccine effectiveness against medically attended RSV outcomes in adults aged ≥60 years was consistently substantial, though estimates varied by setting, season, and network.19
In a multi-state EHR network study of emergency department (ED) encounters over one RSV season, combined use of Arexvy (GSK) and Abrysvo (Pfizer) was associated with effectiveness 77% (95% CI, 70-83) against RSV-associated ED encounters, and effectiveness 81% (95% CI, 52-92) against severe outcomes (RSV-associated ICU admission or death).20
In hospitalized adults (19-state network) in which the vaccine product was not identified, vaccine effectiveness against RSV-associated hospitalization was 75% (95% CI, 50-87). 16) A separate national EHR analysis spanning all 50 US states similarly estimated effectiveness in the mid-70% range across syndromic and severity strata in the overall ≥60-year population (with products including Arexvy [GSK] and Abrysvo [Pfizer]): 75.1% (95% CI, 73.6-76.4) against ARI, 75.8% (95% CI, 73.2-78.1) against ED/urgent care (ED/UC) encounters, and 75.5% (95% CI, 73.1-77.6) against hospitalization.21
In a US Veterans target trial emulation (matched vaccinated vs unvaccinated), vaccine effectiveness estimates were also high, with most vaccinated participants receiving Abrysvo (Pfizer) or Arexvy (GSK): 78.1% for RSV infection beginning 14 days after index date, 78.7% for ED/UC encounters, and 80.3% for hospitalization.22 In a Kaiser Permanente Southern California analysis restricted to Abrysvo (Pfizer), estimated effectiveness against RSV-LRTD over one season was 89% (95% CI, 52-97).23
Over two RSV seasons in the IVY Network, overall effectiveness against RSV-associated hospitalization was 58% (95% CI, 45-68). When product type could be evaluated, effectiveness estimates were similar between Arexvy (GSK) and Abrysvo (Pfizer): 64% (95% CI, 47-76) vs 61% (95% CI, 41-74), respectively.24
EFFECTIVENESS IN IMMUNOCOMPROMISED ADULTS AND TRANSPLANT SUBGROUPS
Effectiveness in immunocompromised adults re-mained clinically meaningful in some datasets but was more variable than in the overall population. In the multi-state EHR network study, effectiveness against hospitalization among immunocompromised adults (primarily vaccinated with Arexvy [GSK] or Abrysvo [Pfizer]) was 73% (95% CI, 43-85).18 In the national EHR analysis, immunocompromised adults had effectiveness estimates of 70.4% (95% CI, 67.8-72.7) against ARI, 73.9% (95% CI, 69.3-77.8) against ED/UC encounters, and 69.5% (95% CI, 65.3-73.1) against hospitalization.21
Within transplant subgroups, heterogeneity was pronounced. Solid organ transplant recipients had effectiveness 73.4% (95% CI, 61.9-81.4) against ARI, whereas hematopoietic stem cell transplant (HSCT) recipients had lower estimates: 33.4% (95% CI, 12.3-49.4) against ARI, 58.4% (95% CI, 37.4-72.8) against ED/UC encounters, and 55.9% (95% CI, 40.0-72.3) against hospitalization.21
By contrast, in the IVY Network analysis over two seasons, effectiveness in immunocompromised adults (receiving a mix of products including Arexvy [GSK], Abrysvo [Pfizer], and mResvia [Moderna]) was 30% (95% CI,−9-55), underscoring variability by design, outcome, and population.24
SAFETY
COMPANY-PROVIDED SAFETY PROFILES FROM RANDOMIZED TRIALS
Across platforms, reactogenicity was consistently higher in vaccine recipients, while serious adverse event rates were generally balanced between vaccine and placebo groups in pivotal trials.
For Abrysvo (RSVpreF; Pfizer), the adult challenge study reported more local injection reactions in vaccine recipients and no serious adverse events in either arm.5 In RENOIR (≥60 years), local reactions occurred in 12% vs 7% (vaccine vs placebo); systemic events were similar (27% vs 26%); and SAEs occurred in 2.3% of participants in both groups.6
For Arexvy (RSVPreF3 OA + AS01; GSK), local-site reactions were reported in 60.9% vs 9.3% and fatigue in 33.6% vs 16.1% (vaccine vs placebo); unsolicited adverse events were 1.4% vs 1.4%. (4) In the three-season study, <1% of SAEs were considered related, and five related deaths were reported across arms as adjudicated in the trial reporting.11
For mResvia (mRNA-1345; Moderna), local reactions were reported in 58.7% vs 16.2% and systemic reactions in 47.7% vs 32.9% (vaccine vs placebo); SAEs occurred in 2.8% of participants in both groups.12
For the Janssen investigational Ad26.RSV.preF/RSV preF protein vaccine, local reactions were 37.9% vs 8.4% and systemic reactions 41.4% vs 16.4% (vaccine vs placebo); SAEs were 4.6% vs 4.7%. (9) Multi-season follow-up reported comparable SAE rates between groups by season.14
For the Bavarian Nordic investigational MVA-BN-RSV vaccine, the challenge study reported local side effects in 88.9% vs 37.8% and SAEs in 80.6% vs 51.4% (vaccine vs placebo), with one myocarditis reported in each group.16 In the phase 3 older-adult study, unsolicited adverse events were 6.5% vs 6.5% and SAEs were 5.5% vs 4.7% (vaccine vs placebo).17
A meta-analysis of randomized trials in older adults supported these trial-level observations, reporting no significant differences in SAEs between RSV vaccines and placebo across pooled data.25
REAL-WORLD SAFETY PROFILE AND COMPARATIVE SIGNALS
Real-world observational evaluations have fo-cused on rare, clinically important events that are difficult to detect reliably in trials, particularly neurologic syndromes. In a large United States (US) electronic hospital record (HER)-based analysis assessing both effectiveness and safety among adults aged ≥60 years, GBS and immune thrombocytopenia (ITP) outcomes were evaluated with product attribution and included recipients of Arexvy (GSK) and Abrysvo (Pfizer). The study concluded that there was an estimated excess risk of GBS at the population level, while no excess risk of ITP was detected for either manufacturer.21 For all vaccine recipients (64.7% [3,070,888 of 4,746,518] received RSVPreF3+AS01), the estimated excess was 11.2 GBS cases per 1,000,000 vaccines administered; the estimated excess associated with Abrysvo (Pfizer) was 18.2 per 1,000,000, and the estimated excess associated with Arexvy (GSK) was 5.2 per 1,000,000 vaccinations.21
Consistent with these observational findings, an updated evidence synthesis reported a higher risk of GBS associated with Abrysvo (Pfizer) (18.2 excess cases per 1 million doses; 95% CI, 9.8-23.3) and no clear excess with Arexvy (GSK) (incidence rate ratio 1.5; 95% CI, 0.9-2.2). This synthesis also reported no meaningful difference in the odds of myocardial infarction between vaccinated and unvaccinated groups (odds ratio 1.11; 95% CI, 0.72-1.71).25
Taken together, randomized trials consistently demonstrated increased short-term local and systemic reactogenicity without major imbalances in serious adverse events, whereas real-world analyses identified small excess risks for rare neurologic outcomes (notably GBS) that may vary by product, with no consistent signal for ITP across manufacturers in the cited data.
DISCUSSION
This narrative review demonstrates that licensed RSV vaccines in adults, especially those aged 60 years and older, achieve moderate-to-high efficacy against RSV-associated lower respiratory tract disease.6-8,10-13
Across pivotal trials in older adults, RSV vaccine efficacy varied by product, season, and case-definition stringency. For Pfizer’s RSVpreF (Abrysvo), first-season efficacy ranged from 66.7% for RSV-LRTD using a ≥2 signs/symptoms definition to 85.7% using ≥3 signs/symptoms, with 62.1% efficacy against RSV-ARI; over two seasons, overall efficacy for RSV-LRTD using ≥2 signs/symptoms was 57.5%, while age-stratified point estimates using more stringent criteria were higher but imprecise in older strata.6,7 For GSK’s adjuvanted RSVPreF3 OA (Arexvy), first-season efficacy was 82.6% against RSV-LRTD and 94.1% against severe RSV-LRTD; efficacy attenuated in later seasons (67.2% in season two and 62.9% across three seasons), while remaining clinically meaningful and showing cross-subtype protection despite an RSV-A-based antigen.8-11 Moderna’s mRNA-1345 also demonstrated high efficacy over one year (83.7% against RSV-LRTD using ≥2 signs/symptoms and 82.4% using ≥3 signs/symptoms), with 68.4% efficacy against RSV-ARI. These results collectively support a practical efficacy range of approximately 57% to 94% for RSV-LRTD-related endpoints, with higher point estimates generally observed for more stringent or severe disease definitions and lower estimates in broader or longer follow-up analyses.6-12
Real-world effectiveness studies during early rollout seasons largely corroborate these trial findings. Multiple U.S. analyses reported substantial effectiveness against RSV-associated hospitalizations, emergency department encounters, and other medically attended outcomes in adults aged 60 years and older, and product-specific estimates, when available, suggest broadly comparable performance of the two most widely used products for hospitalization endpoints in routine practice.20-24 Two-season analyses reported lower effectiveness against hospitalization than many single-season estimates, consistent with waning immunity, changes in RSV epidemiology, and differences in vaccinated populations over time.24 Effectiveness in immunocompromised adults was more variable and often less precise than in the overall older-adult population, and transplant subgroup estimates in particular suggested heterogeneity that likely reflects differences in immune suppression intensity and mechanisms.21,24
U.S. Food and Drug Administration materials for COVID-19 licensure-supporting trials used a benchmark of vaccine efficacy with a point estimate of at least 50% and an appropriately alpha-adjusted lower bound of the confidence interval of at least 30%.26 Although these thresholds are COVID-19-specific, they provide context suggesting that many RSV efficacy estimates in older adults are clinically meaningful and are reinforced by real-world reductions in hospitalization and other severe outcomes.
A comparison with updated COVID-19 vaccination is most informative when framed around preventing severe outcomes in high-risk adults rather than preventing all infection. Centers for Disease Control and Prevention interim analyses for September 2023 through January 2024 showed that the updated 2023-2024 COVID-19 vaccination provided meaningful protection against COVID-19-associated emergency department/urgent care encounters and hospitalization in adults, with effectiveness varying by time since vaccination.27 Similarly, RSV vaccines show substantial real-world effectiveness against hospitalization and other severe outcomes in older adults during early seasons, while multi-season estimates and subgroup analyses point to the need for ongoing evaluation of durability and performance in immunocompromised populations.
For intensive care unit (ICU) admission, respiratory failure, and in-hospital mortality, the evidence base is more limited than for RSV-LRTD or hospitalization. Pivotal trials were generally not powered to estimate protection against these rare endpoints as stand-alone outcomes, and observational studies often report a composite of critical illness outcomes that combine ICU admission and/or death rather than providing precise, component-specific estimates for ICU admission, mechanical ventilation, and mortality separately.20-24
Overall, the available evidence indicates that adult RSV vaccines have good efficacy against RSV-associated lower respiratory tract disease and demonstrate substantial real-world effectiveness against severe, medically attended outcomes. However, further prospective, adequately powered studies using standardized definitions are needed to determine whether vaccination reduces the risk of respiratory failure requiring mechanical ventilatory support, ICU admission, and in-hospital mortality as distinct endpoints.
CONCLUSION
In adults aged ≥60 years, current RSV vaccines provide clinically meaningful protection in trials and substantial real-world effectiveness against severe outcomes, including hospitalization. Evidence in immunocompromised adults supports the benefit but is more variable and currently insufficient for confident product-level ranking, particularly in highly immunosuppressed subgroups. Multi-season attenuation suggests booster strategies merit targeted evaluation, and safety data support use with continued monitoring for rare neurologic events.
REFERENCES
- Falsey AR, Hennessey PA, Formica MA, et al. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005;352(17):1749–59. (In eng). DOI: 10.1056/NEJMoa043951.
- Shi T, Denouel A, Tietjen AK, et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J Infect Dis. 2020;222(Suppl 7):S577–83. (In eng). DOI: 10.1093/infdis/jiz059.
- Savic M, Penders Y, Shi T, et al. Respiratory syncytial virus disease burden in adults aged 60 years and older in high-income countries: A systematic literature review and meta-analysis. Influenza Other Respir Viruses. 2023;17(1):e13031. (In eng). DOI: 10.1111/irv.13031.
- McLaughlin JM, Khan F, Begier E, et al. Rates of Medically Attended RSV Among US Adults: A Systematic Review and Meta-analysis. Open Forum Infect Dis. 2022;9(7):ofac300. (In eng). DOI: 10.1093/ofid/ofac300.
- Schmoele-Thoma B, Zareba AM, Jiang Q, et al. Vaccine Efficacy in Adults in a Respiratory Syncytial Virus Challenge Study. N Engl J Med. 2022;386(25):2377–86. (In eng). DOI: 10.1056/NEJMoa2116154.
- Walsh EE, Pérez Marc G, Zareba AM, et al. Efficacy and Safety of a Bivalent RSV Prefusion F Vaccine in Older Adults. N Engl J Med. 2023;388(16):1465–77. (In eng). DOI: 10.1056/NEJMoa2213836.
- Walsh EE, Marc GP, Falsey AR, et al. RENOIR Trial — RSVpreF Vaccine Efficacy over Two Seasons. New England Journal of Medicine. 2024;391(15):1459–60. DOI: 10.1056/NEJMc2311560.
- Papi A, Ison MG, Langley JM, et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine in Older Adults. N Engl J Med. 2023;388(7):595–608. (In eng). DOI: 10.1056/NEJMoa2209604.
- Ison MG, Papi A, Athan E, et al. Efficacy and Safety of Respiratory Syncytial Virus (RSV) Prefusion F Protein Vaccine (RSVPreF3 OA) in Older Adults Over 2 RSV Seasons. Clin Infect Dis. 2024;78(6):1732–44. (In eng). DOI: 10.1093/cid/ciae010.
- Feldman RG, Antonelli-Incalzi R, Steenackers K, et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine Is Efficacious in Older Adults With Underlying Medical Conditions. Clin Infect Dis. 2024;78(1):202–9. (In eng). DOI: 10.1093/cid/ciad471.
- Ison MG, Papi A, Athan E, et al. Efficacy, safety, and immunogenicity of the AS01(E)-adjuvanted respiratory syncytial virus prefusion F protein vaccine (RSVPreF3 OA) in older adults over three respiratory syncytial virus seasons (AReSVi-006): a multicentre, randomised, observer-blinded, placebo-controlled, phase 3 trial. Lancet Respir Med. 2025;13(6):517–29. (In eng). DOI: 10.1016/s2213-2600(25)00048-7.
- Wilson E, Goswami J, Baqui AH, et al. Efficacy and Safety of an mRNA-Based RSV PreF Vaccine in Older Adults. N Engl J Med. 2023;389(24):2233–44. (In eng). DOI: 10.1056/NEJMoa2307079.
- Falsey AR, Williams K, Gymnopoulou E, et al. Efficacy and Safety of an Ad26.RSV.preF-RSV preF Protein Vaccine in Older Adults. N Engl J Med. 2023;388(7):609–20. (In eng). DOI: 10.1056/NEJMoa2207566.
- Falsey AR, Hosman T, Bastian AR, et al. Long-term efficacy and immunogenicity of Ad26.RSV.preF-RSV preF protein vaccine (CYPRESS): a randomised, double-blind, placebo-controlled, phase 2b study. Lancet Infect Dis. 2024;24(9):1015–24. (In eng). DOI: 10.1016/s1473-3099(24)00226-3.
- Tamura H, Momose A, Takato Y, et al. Phase 3 study of an Ad26.RSV.preF/RSV preF protein vaccine to evaluate the prevention efficacy of RSV-mediated lower tract disease, immunogenicity and safety in Japanese adults. Respir Investig. 2025;63(4):560-68. (In eng). DOI: 10.1016/j.resinv.2025.04.016.
- Jordan E, Kabir G, Schultz S, et al. Reduced Respiratory Syncytial Virus Load, Symptoms, and Infections: A Human Challenge Trial of MVA-BN-RSV Vaccine. J Infect Dis. 2023;228(8):999-1011. (In eng). DOI: 10.1093/infdis/jiad108.
- Jordan E, Jenkins V, Silbernagl G, et al. A multivalent RSV vaccine based on the modified vaccinia Ankara vector shows moderate protection against disease caused by RSV in older adults in a phase 3 clinical study. Vaccine. 2024;42(26):126427. (In eng). DOI: 10.1016/j.vaccine.2024.126427.
- Zeng B, Liu X, Yang Q, et al. Efficacy and safety of vaccines to prevent respiratory syncytial virus infection in infants and older adults: a systematic review and meta-analysis. Int J Infect Dis. 2024;146:107118. (In eng). DOI: 10.1016/j.ijid.2024.107118.
- Surie D, Self WH, Zhu Y, et al. RSV Vaccine Effectiveness Against Hospitalization Among US Adults 60 Years and Older. JAMA. 2024;332(13):1105-7. (In eng). DOI: 10.1001/jama.2024.15775.
- Payne AB, Watts JA, Mitchell PK, et al. Respiratory syncytial virus (RSV) vaccine effectiveness against RSV-associated hospitalisations and emergency department encounters among adults aged 60 years and older in the USA, October, 2023, to March, 2024: a test-negative design analysis. Lancet. 2024;404(10462):1547–59. (In eng). DOI: 10.1016/s0140-6736(24)01738-0.
- Fry SE, Terebuh P, Kaelber DC, et al. Effectiveness and Safety of Respiratory Syncytial Virus Vaccine for US Adults Aged 60 Years or Older. JAMA Netw Open. 2025;8(5):e258322. (In eng). DOI: 10.1001/jamanetworkopen.2025.8322.
- Bajema KL, Yan L, Li Y, et al. Respiratory syncytial virus vaccine effectiveness among US veterans, September, 2023 to March, 2024: a target trial emulation study. Lancet Infect Dis. 2025;25(6):625–33. (In eng). DOI: 10.1016/s1473-3099(24)00796-5.
- Tartof SY, Aliabadi N, Goodwin G, et al. Estimated Vaccine Effectiveness for Respiratory Syncytial Virus-Related Lower Respiratory Tract Disease. JAMA Netw Open. 2024;7(12):e2450832. (In eng). DOI: 10.1001/jamanetworkopen.2024.50832.
- Surie D, Self WH, Yuengling KA, et al. RSV Vaccine Effectiveness Against Hospitalization Among US Adults Aged 60 Years or Older During 2 Seasons. JAMA. 2025;334(16):1442–51. DOI: 10.1001/jama.2025.15896.
- Scott J, Abers MS, Marwah HK, et al. Updated Evidence for Covid-19, RSV, and Influenza Vaccines for 2025-26. New England Journal of Medicine. 2025;393(22):2221-42. DOI: 10.1056/NEJMsa2514268.
- Halperin SA, Ye L, MacKinnon-Cameron D, et al. Final efficacy analysis, interim safety analysis, and immunogenicity of a single dose of recombinant novel coronavirus vaccine (adenovirus type 5 vector) in adults 18 years and older: an international, multicentre, randomised, double-blinded, placebo-controlled phase 3 trial. Lancet. 2022;399(10321):237-48. (In eng). DOI: 10.1016/s0140-6736(21)02753-7.
- DeCuir J, Payne AB, Self WH, et al. Interim Effectiveness of Updated 2023-24 (Monovalent XBB.1.5) COVID-19 Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalization Among Immunocompetent Adults Aged ≥18 Years-VISION and IVY Networks, September 2023-January 2024. MMWR Morb Mortal Wkly Rep. 2024;73(8):180-88. (In eng). DOI: 10.15585/mmwr.mm7308a5.
Article citation: Puchongmart C, Bueso A, Holguin S, Wanichwecharungruang N, Suriyathumrongkul N, Sodsri T, Thiravetyan B. Efficacy, effectiveness, and safety of respiratory syncytial virus vaccines in adults: Evidence from clinical trials and real-world effectiveness studies. The Southwest Journal of Medicine. 2026;14(60):25-39
From: Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas (CP, AB, SH, NW, NS, TS, BT)
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.