Abstract
The use of robotic bronchoscopy with EBUS and pulsed electric field ablation for metastatic melanoma in a lung nodule
David H. Lindner DO, Danielle Sanchez MD
Corresponding author: Danielle Sanchez
Contact Information: Daniellesd96@gmail.com
DOI: 10.12746/swjm.v14i60.1663
ABSTRACT
Malignant melanoma is one of the lethal forms of cancer, with approximately 8,290 deaths expected in 2024.1 Information available on melanomas of unknown primary origin remains limited. A review by Song theorized that the most likely hypothesis of its etiology is immune-mediated regression of the primary after metastasis has occurred.3 Our case represents a patient with metastatic melanoma found in both pancreatic and lung tissues. The pancreatic biopsy results were consistent with malignant melanoma. Pancreatic melanoma is more commonly a site of metastasis than a primary tumor, and in this case, the presentation was nonspecific. Regardless, malignant melanoma is treated by immunomodulator therapy involving PD1 inhibitors alone or in combination with ipilimumab. That being said, the patient was considered for a biopsy of the lung nodule with Pulsed Electric Field ablation as a concomitant treatment approach by the oncology team.
After undergoing the biopsy but before starting treatment, the Pulse Electrical Field was used for its properties of targeting the tumor site with its abscopal effect, leading to a process called pyroptosis. Pyroptosis leads to inflammatory vesicles filled with damage-associated molecular patterns (DAMPs), which are later released from the cell via gadermin D, GSDMD pores to elicit an immune response.8 Treatment was successful at 8-month follow-up CT scan, which showed no recurrence of the lesions. In summary, PEF leads to tumor shrinkage both within the targeted treatment area and at distant sites outside the treatment field. This case is the first to use pulse electrical field ablation as an adjunct to immunotherapy for malignant lesions.
Keywords: Endobronchial, melanoma, Pulse electrical field ablation, lung nodule, abscopal
CASE
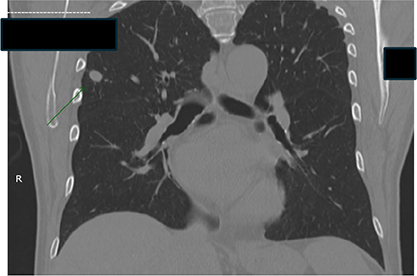
A 75-year-old male with no past medical history who presented to the emergency department with shortness of breath. His evaluation revealed atrial flutter, for which he underwent transesophageal echocardiography (TEE)-guided cardioversion that was unsuccessful, followed by cardiac ablation. At the time, chest imaging demonstrated a pulmonary nodule suspicious of metastatic disease (Figure 1). Additional abdominal imaging revealed a lesion in the tail of the pancreas. This was a low-attenuation mass measuring 3.5 × 2.2 cm. There were no adjacent pathologic abnormalities or appreciable hepatic masses. Chest imaging also demonstrated a well-defined 13 × 9 mm pulmonary nodule in the right upper lobe and a 7 mm nodule in the left upper lobe, with only mild mediastinal adenopathy (Figure 2). Both pulmonary nodules were suspicious for metastatic disease. The patient underwent a pancreatic biopsy on January 3, 2025, which revealed a malignant neoplasm with extensive necrosis. Immunostains were positive for synaptophysin and chromogranin, highlighting pancreatic islets of Langerhans. Ki-67 proliferative index was low within neuroendocrine cells in the islets, arguing against pancreatic origin. Tumor cells were diffusely positive for SOX10 and S100, and negative for Melan-A, AE1/AE3 CK8/18, CK7, CK20, CDX2, synaptophysin, chromogranin, CD3, and CD20. Rare tumor cells are positive for HMB45. The Ki-67 proliferative index was approximately 40% based on semiquantitative manual scoring. The immunoprofile was nonspecific; however, the findings were consistent with malignant melanoma. Pancreatic melanoma is usually considered metastatic, whereas primary pancreatic melanoma is exceedingly rare. The diagnosis of pancreatic melanoma, particularly the distinction between primary and metastatic disease, remains challenging. Melanoma arises from melanocytes and originates from cutaneous, ocular, mucosal, and unknown primary sites in approximately 91.2%, 5.2%, 1.3%, and 2.2% of cases, respectively.2

Month 1
Figure 1. CT chest on presentation, the largest nodule is 1 cm, seen on display.
Month 3
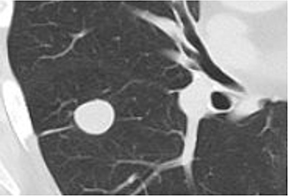
Figure 2. CT chest before bronchoscopy, showing a 13 × 9 mm right upper lobe lesion in the lateral series (image number 54), compared with a 12 × 10 mm lesion previously.
In this case, the origin of the pancreatic melanoma is unknown. Clinical evaluation was unrevealing for a primary site. The diagnosis of primary pancreatic melanoma is uncommon. Nakamura published a review of 76 reported cases. If primary in origin, pancreatic melanoma may arise from ectopic melanocytes, migrated neural crest cells, or other neural-derived cells within the pancreas.4
Because of the metastatic nature of the disease, surgical resection of the pancreatic lesion was not offered, as a survival benefit has been demonstrated only with complete surgical resection.5 Treatment of metastatic melanoma has focused primarily on immunotherapy and targeted therapy. The patient was referred to NCH Pulmonary Medicine for consideration of biopsy of the 13 × 9 mm right upper lobe density and consideration of Pulsed Electric Field ablation to be utilized as a concomitant treatment approach by the oncology team. Focal ablation techniques are a valuable, minimally invasive tool for the management of metastatic tumors.6 There is also evidence that supports immune-mediated off-target, abscopal effects of Pulsed Electric Field ablation.7
After obtaining consent for the biopsy and planned ablation, the patient underwent a bronchoscopy with biopsy of the lesion and planned pulsed electric field ablation (Figure 3).
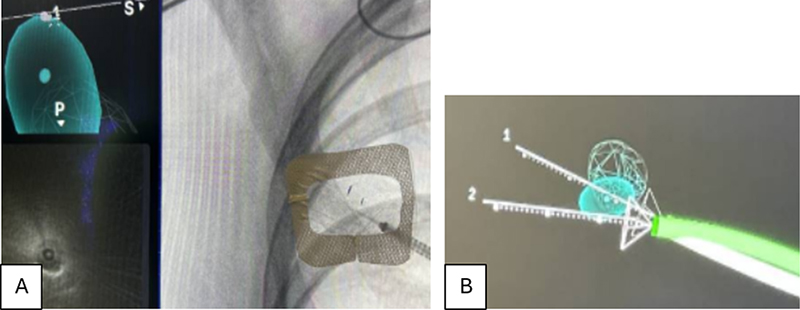
Figure 3. A. Using Intuitive Ion TM robotic bronchoscopy with radial EBUS and CIOS TM Cone Beam localization, fine needle aspiration was completed, and ROSC demonstrated ROSC lesional tissue consistent with the known malignancy. B. Vector analysis for the PEF was completed, and ablation using two vectors and 5 ablation treatments, each at 5 minutes.
The patient tolerated the procedure well without adverse events and was discharged home following the procedure. Final pathology of the RUL biopsy demonstrated fragments of malignant neoplastic cells. These tumor cells were morphologically consistent with the tumor cells seen in previous pancreatic biopsies and demonstrated diffuse positivity for SOX10, S100, and PRAME; however, negative for Melan-A, HMB45, and AE1/AE3. The immunoprofile was nonspecific but was similar to the findings of the previous biopsy. The patient was seen in follow-up by Medical Oncology and was started on pembrolizumab without complications. He returned for follow-up 3 months after PEF. Clinically, he was asymptomatic and maintained an excellent performance status,with no further weight loss, shortness of breath, or cough.
Reimaging of the CT chest of the RUL lesion demonstrated marked improvement following ablation. The PET Scan performed in Apr 2025 demonstrated a new faintly FDG-avid 1.9 × 1.8 cm peri-fissural nodule in the superior segment of the right lower lobe with SUV Max of 1.7, corresponding to a previously identified 0.7 cm nodule on November 10, 2024. The lateral right upper lobe nodule was also faintly FDG-avid but had decreased in size to 0.8 cm from 1.1 cm on January 8, 2025. There was also an interval resolution of a fissural nodule, which had been seen on the January 8, 2025 imaging (Figure 4).
Month 3
Figure 4. Lung nodule before undergoing bronchoscopy with pulse electrical field ablation.
PET scan performed on January 30, 2025, demonstrated an FDG-avid necrotic pancreatic mass, pancreatic body tail 5.6 × 4.1 cm, with an SUV of 7.9. Additional findings included a necrotic 3.7 × 2.6 cm mesenteric soft tissue lesion with a maximum SUV of 6.8 and focal FDG uptake in the left upper quadrant corresponding to the small bowel, with a maximum SUV of 15.1.
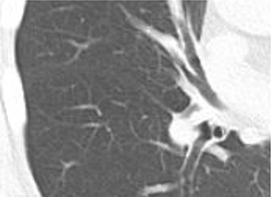
The patient was subsequently initiated on Pembrolizumab 200 mg every 21 days and completed five cycles between February 5, 2025, and April 30, 2025. Repeat PET on April 25, 2025, demonstrated interval enlargement of the pancreatic mass. The centrally necrotic pancreatic mass measured 6.8 × 4.9 cm with a maximum SUV of 10.6, increased from 5.3 × 3.1 cm on November 11, 2024, when remeasured in the same plane. At that time, the findings were considered most consistent with pseudoprogression. The patient otherwise tolerated treatment well. He developed immune-mediated hepatitis secondary to pembrolizumab, which was managed with prednisone 10 mg daily and remained ongoing. Repeat PET/CT performed on November 19, 2025, demonstrated complete resolution of the pulmonary nodules (Figure 5). The necrotic pancreatic body/tail mass measured 9.3 cm with a maximum SUV of 15, compared with a previous SUV of 17.
Month 6
Figure 5. Post pulse electrical field ablation nodule no longer presents.
DISCUSSION
This case highlights the successful use of a pulse electrical field in combination with immunotherapy for the ablation of a metastatic melanoma from a pulmonary nodule
ACKNOWLEDGMENTS
Steven Newman, MD, Oncology.
REFERENCES
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7-30.
- Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. Cancer. 1998;83:1664-78.
- Song Y, Karakousis GC. Melanoma of unknown primary. J Surg Oncol. 2019;119:232-41.
- Nakamura Y, Yamada R, Kaneko M, et al. Isolated pancreatic metastasis from malignant melanoma: a case report and literature review. Clin J Gastroenterol. 2019.
- Nikfarjam M, Evans P, Christophi C. Pancreatic resection for metastatic melanoma. HPB (Oxford). 2003;5(3):174-9.
- Jimenez M, Ng C, Iding J, et al. Single-needle delivery of pulsed electric fields (PEF) energy to early-stage non-small cell lung cancer (NSCLC): feasibility and safety near sensitive structures in the INCITE ES study. J Vasc Interv Radiol. 2023;34(3 Suppl):S71-S72.
- Pastori C, Nafie EHO, Wagh MS, et al. Pulsed electric field ablation versus radiofrequency thermal ablation in murine breast cancer models: anticancer immune stimulation, tumor response, and abscopal effects.
- Batista Napotnik T, Polajžer T, MiklavCiC D. Cell death due to electroporation: a review. Bioelectrochemistry. 2021;141:107871.
Article citation: Lindner D, Sanchez D. The use of robotic bronchoscopy with EBUS and pulsed electric field ablation for metastatic melanoma in a lung nodule. The Southwest Journal of Medicine. 2026;14(60):63–66
From: Department of Pulmonary, Critical Care, Sleep Medicine, Naples Comprehensive Health, Naples, FL (DL) Graduate Medical Education, Naples, FL (DS)
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.