Abstract
The correlation between brain natriuretic peptide levels and six-minute walk distances in patients with heart failure with a preserved ejection fraction
Gaspar Del Rio-Pertuz MD, Natnicha Leelaviwat MD, Mitchel Devolder BS, Erwin Argueta MD, Kenneth Nugent MD
Corresponding author: Kenneth Nugent
Contact Information: Kenneth.Nugent@ttuhsc.edu
DOI: 10.12746/swjm.v14i60.1677
ABSTRACT
Patients with heart failure with preserved ejection fractions (HFpEF) often have complex presentations and have significant comorbidity. This diagnosis occurs more frequently in older women with hypertension, diabetes, and obesity. Their cardiac disorder and their comorbidity limit their physical activity levels. Management of these patients requires regular follow-up with adjustment of the medication, if needed. Trends in simple laboratory tests, such as a brain natriuretic peptide levels, could help determine responses to treatment and prognosis. This study analyzed the correlation between BNP levels and six-minute walk test distances in patients with established HFpEF. The study included 21 patients with a mean age of 61.1 ± 9.1 years. All patients had hypertension, 11 patients had diabetes, and 10 patients had chronic kidney disease. The mean BNP level was 490.0 ± 653.5 pg/mL. The mean six-minute walk distance was 300.4 meters ± 120.8 meters. There was no significant correlation between the six-minute walk distance and the BNP. Consequently, this study demonstrates that routine measurement of BNP levels does not provide significant information about the patient’s overall physical performance level.
Keywords: Heart failure with preserved ejection fraction, brain natriuretic peptide, six-minute walk distance
INTRODUCTION
The management of patients with heart failure with preserved ejection fractions (HFpEF) presents a complex set of clinical problems to physicians. The initial problem involves establishing a working diagnosis since many of these patients have several comorbid conditions which could explain their symptoms.1 The second problem involves establishing a treatment regimen. The third problem involves the identification of testing criteria that help determine responses to treatment and possibly predict prognosis. Clinical questionnaires, such as a New York Heart Association classification, can help determine the level of impairment, but the results on this questionnaire reflect the overall clinical condition of the patient and may not necessarily reflect a specific cardiac limitation. Six-minute walk tests provide a quantitative result that can establish the patient’s level of overall impairment. However, this testing requires additional clinic time and expense and is not used routinely in many cardiology clinics. Serial measurements of brain natriuretic peptide (BNP) levels can potentially determine response to treatment and predict prognosis. These measurements become more valuable if they correlate with six-minute walk test results. This pilot study prospectively measured BNP levels and six-minute walk tests in patients with HFpEF followed in a cardiology clinic.
METHOD
Patients followed in cardiology clinics at Texas Tech University Health Sciences Center clinics in Lubbock, Texas, were reviewed to determine if they had HFpEF. Study coordinators explained the project to ambulatory patients with this diagnosis and obtained informed consent. Each patient then had blood drawn for a BNP level and performed a six-minute walk test. Clinic records were reviewed to collect information about demographics, medication, comorbidity, and functional status. Patients received a small stipend to support travel expenses. The Institutional Review Board at Texas Tech University Health Sciences Center approved the study (L22-070). The Clinical Research Institute at Texas Tech University Health Sciences Center in Lubbock, Texas, provided support for the study, and the Graduate Medical Education office on the Lubbock campus provided financial support for this pilot project.
RESULTS
This study included 21 patients with 11 women and 10 men. The median age was 60.0 years old with an interquartile range of 13 years (Table 1). Race and ethnic distribution included three African American patients, eight Hispanic patients, nine White patients, and one patient with no recorded designation. The median body mass index was 36.2 kg/m2 with an interquartile range of 9.2 kg/m2. These patients have had the clinical diagnosis of HFpEF for 24.0 months with an interquartile range of 43.3 months.
Table 1. Demographics of Study Subjects
| Variable |
Overall (N = 21) |
| Sex |
| F |
11 (52%) |
| M |
10 (48%) |
| Age (years) |
| Mean (SD) |
61.14 (9.05) |
| Median (IQR) |
60.00 (13.00) |
| Min, Max |
46.00, 82.00 |
| Race/Ethnicity |
| African American |
3 (15%) |
| Hispanic |
8 (40%) |
| White |
9 (45%) |
| Unknown |
1 |
| Height (cm) |
| Mean (SD) |
168.86 (10.91) |
| Median (IQR) |
168.00 (18.00) |
| Min, Max |
152.00, 188.00 |
| Weight (kg) |
| Mean (SD) |
107.11 (19.63) |
| Median (IQR) |
105.86 (30.93) |
| Min, Max |
67.86, 134.72 |
| BMI (kg/m2) |
| Mean (SD) |
37.73 (7.51) |
| Median (IQR) |
36.22 (9.20) |
| Min., Max |
28.25, 54.66 |
The patients had the following comorbid conditions: hypertension (n-21), diabetes (n-11), chronic kidney disease (n-10, III a & b), coronary artery disease (n-six), and asthma/COPD (n-4). Current medications included diuretics (n-17), spironolactone (n-9), angiotensin-converting enzyme inhibitors (n-12), angiotensin receptor blockers (n-2), beta blockers (n-15), sacubitril/valsartan (n-4), sodium-glucose cotransporter-2 (SGLT2) inhibitors (n-10). One patient used supplemental oxygen.
Clinical variables (heart rate and levels of dyspnea and fatigue) reported during the six-minute walk tests are reported in Table 2. The median six-minute walk distance was 304.8 meters with an interquartile range of 189 meters (Table 3). The shortest six-minute walk distance was 121.9 meters, and the longest distance was 501.0 meters. The median BNP level was 216.0 pg/mL with an interquartile range of 313.0 pg/mL. The lowest BNP level was 49.0 pg/mL, and the highest level was 2710 pg/mL. The correlation between the six-minute walk distance and the BNP level was 0.052 with a P value of 0.82. The figure plots BNP levels against the six-minute walk distances.
Table 2. Clinical Variables (Pre-post walk measurements)
| Variable |
Pre-Test |
Post-Test |
| Heart rate, beats per minute |
| Mean (SD) |
71.62 (10.64) |
85.00 (14.67) |
| Median (IQR) |
71.00 (11.00) |
84.00 (19.00) |
| Min, Max |
51.00, 95.00 |
63.00, 126.00 |
| Dyspnea, Borg scale |
| Mean (SD) |
0.43 (1.36) |
2.95 (2.91) |
| Median (IQR) |
0.00 (0.00) |
2.00 (6.00) |
| Min., Max. |
0.00, 5.00 |
0.00, 9.00 |
| Fatigue, Borg scale |
| Mean (SD) |
0.90 (1.81) |
3.10 (2.90) |
| Median (IQR) |
0.00 (0.00) |
3.00 (6.00) |
| Min, Max |
0.00,6.00 |
0.00,8.00 |
| SpO2, % |
| Mean (SD) |
94.43 (2.27) |
93.19 (4.82) |
| Median (IQR) |
94.00 (3.00) |
95.00 (5.00) |
| Min, Max |
90.00, 99.00 |
81.00, 99.00 |
| Dyspnea (0 vs >0) |
| 0 |
19 (90%) |
6 (29%) |
| Greater Than 0 |
2 (9.5%) |
15 (71%) |
| Fatigue (0 vs >0) |
| 0 |
16 (76%) |
7 (33%) |
| Greater Than 0 |
5 (24%) |
14 (67%) |
DISCUSSION
This study demonstrates that there is no correlation between the six-minute walk distances and the BNP levels in these patients with HFpEF. Consequently, this simple laboratory test does not provide much information about a patient’s overall physical capacity, and determining physical activity performance in these patients will depend on actual testing with six-minute walk tests or cardiopulmonary exercise testing.
The physical activity level/performance in these patients reflects their underlying cardiac disease, the effect of various comorbid conditions, such as obesity, and possibly chronic deconditioning. These factors potentially limit any correlation between heart failure status based on BNP levels and physical activity level. Several clinical factors can alter BNP levels.2 Nishikimi and Nakagawa reviewed the factors relevant to the interpretation of plasma BNP levels in heart failure.3 Levels are increased in older patients, female patients, patients with renal dysfunction, patients with atrial fibrillation, inflammation and hyperthyroidism, and patients on sacubitril/valsartan. Obesity is associated with lower levels of BNP, and plasma BNP levels correlate inversely with BMI. Brain natriuretic peptide production and secretion decrease with increasing insulin resistance, which commonly develops in patients with obesity. In addition, there is decreased intracellular pro-BNP processing, which leads to decreases in both NT-proBNP and BNP, and there is increased uptake of BNP in adipocytes secondary to increased NPR-A and NPR-C receptor expression. These authors noted that high levels of uncleaved pro-BNP circulate in the blood and are measured by most BNP assays. Consequently, BNP levels do not necessarily reflect active peptide levels.
In addition, BNP levels fluctuate even if the patient is clinically stable. Maisel et al. analyzed the information from a prospective trial in which patients with heart failure measured BNP and body weight at home.4 Intra-individual BNP dispersion was greater in patients with HFpEF than in patients with HFrEF secondary to rapid fluctuations within a 3-day period. Approximately 10% of patients HFpEF had an increase in BNP more than 2-fold over 3 days. These results indicate that there are daily fluctuations in BNP levels in patients with heart failure, and these fluctuations are greater in patients with HFpEF. Consequently, the measurement of BNP on any given day may not be representative of this patient’s average BNP. Patients with rapid increases in BNP levels are at increased risk for acute decompensated heart failure. In patients with HFpEF, an increase of BNP greater than 200 pg/mL within 3 days and a weight gain of greater than 2 pounds over 3 days were associated with acute decompensation, but the sensitivity was only 60%.
Table 3. Correlation Between BNP and 6-MWT
| 6-MWT Distance (meters) |
Correlation: 0.052
P-value: 0.823 |
Slope: 0.004
95% CI: -0.085, 0.093
P-value: 0.923 |
| Mean (SD), meters |
300.39 (120.82) |
| Median (IQR), meters |
304.80 (189.00) |
| Min, Max, meters |
121.92, 501.00 |
| BNP, pg/mL |
| Mean (SD), pg/mL |
449.00 (653.48) |
| Median (IQR), pg/mL |
216.00 (313.00) |
| Min, Max, pg/mL |
49.00, 2,710.00 |
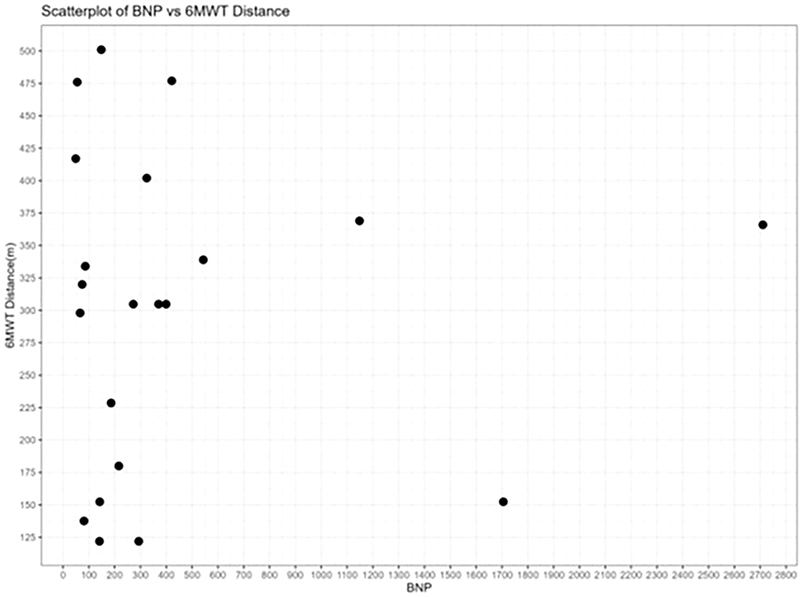
Figure 1. The BNP levels in pg/mL are plotted against six-minute walk distances in meters.
Brain natriuretic peptide levels do not appear to predict prognosis in patients with HFpEF when used to guide therapy. Horiuchi et al. reviewed natriuretic peptide guided therapy in patients with heart failure.5 This approach seems useful in patients with reduced ejection fraction but not in patients with HFpEF. The six-minute walk test distance does predict prognosis in patients with heart failure. Fujimoto classified 513 older patients hospitalized with decompensated heart failure according to their six-minute walk distances performed in the hospital after clinical stabilization.6 The lowest tertile had a distance of 166 m or less. During the follow-up, 90 all-cause deaths occurred. Patients in the lowest tertile had significantly higher event rates. This was true after adjustment for other conventional risk factors. Grundtvig analyzed the outcome of 5519 patients with heart failure in the National Norwegian Heart Failure Registry.7 This registry used the six-minute walk test for prognostic assessment. Patients in the worst six-minute walk distance category had the worst outcomes. The six-minute walk test was a highly significant independent predictor for mortality when entered into a regression model as a continuous variable. The most important predictors for mortality in that model were active cancer in the last 5 years, age, six-minute walk test distance, and natriuretic peptide levels. Zotter-Tufaro et al. analyzed the association between the six-minute walk test distance and outcomes in patients with pulmonary hypertension and HFpEF.8 The six-minute walk test distance was an independent predictor of the outcomes which were either hospitalization for heart failure and/or death for cardiac reasons. In addition, there was a significant inverse correlation between the six-minute walk test distance and the amount of extracellular matrix identified on endomyocardial biopsies.
There is a correlation between the hemodynamic parameters in these patients and their six-minute walk distance. Wolsk et al. analyzed the relationship between the six-minute walk test distance and hemodynamic parameters measured by right heart catheterization.9 At rest, the pulmonary capillary wedge pressure was significantly associated with the six-minute walk test distance. During the light and moderate exercise during catheterization, the mean pulmonary artery pressure was associated with six-minute walk test distance. During peak exercise, the central venous pressure, cardiac index, and pulmonary capillary wedge pressure normalized to cardiac index correlated with the six-minute walk test distance. Consequently, the hemodynamic correlation with the six-minute walk distance depends on the level of exercise performed during right heart catheterization.
Although several factors influence the physical activity level of patients with HFpEF, these patients do benefit from cardiac rehabilitation. Kamiya et al. did a multicenter retrospective study of patients hospitalized with acute heart failure in 15 hospitals in Japan.10 The primary outcome was a composite of all-cause mortality and rehospitalization for heart failure after discharge. This study included 3277 patients; 862 patients participated in outpatient cardiac rehabilitation and were propensity matched to nonparticipants. Cardiac rehabilitation reduced the composite outcome for both all-cause mortality and heart failure-related hospitalization. Participation produced similar results in patients with HFpEF and in frail patients. Sachdev et al. published a scientific statement from the American Heart Association and the American College of Cardiology on supervised exercise training for patients with HFpEF.11 Their analysis indicated that patients with HFpEF had similar or better improvement in exercise capacity than patients with heart failure with reduced ejection fractions. The peak VO2 increased by 14% (2.2 mL/kg/min, from 15.8 to 18.0 mL/kg/min) with rehabilitation.
In summary, in patients with HFpEF, BNP levels seem to have limited value in predicting physical performance and functional status. These patients should be on guideline recommended therapy and will need treatment of comorbidity to the extent possible to reduce symptoms, disease progression, and hospital admissions The evaluation of their clinical status will depend on the use of simple clinical questionnaires, such as a New York Heart Association classification, and physical performance tests, such as the three-minute or six-minute walk test.12 Initial therapeutic goal should focus on reducing fluid overload. These patients likely benefit from cardiac rehabilitation. Their clinical status seems fragile, and they are at risk for acute cardiac decompensation with small 2-pound weight gains. Consequently, routine daily measurement of weight can provide important information to the patient and the clinician.
ACKNOWLEDGMENTS
The Clinical Research Institute at the Texas Tech University Health Sciences Center in Lubbock, Texas, provided support for this project. Milan Bimali PhD provided statistical support.
REFERENCES
- Kittleson MM, Panjrath GS, Amancherla K, et al. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure With Preserved Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2023;81(18):1835-78. (In eng). DOI: 10.1016/j.jacc.2023.03.393.
- Januzzi JL, Myhre PL. The Challenges of NT-proBNP testing in HFpEF: Shooting arrows in the wind. JACC Heart Fail 2020;8(5):382-5. (In eng). DOI: 10.1016/j.jchf.2020.03.003.
- Nishikimi T, Nakagawa Y. Potential pitfalls when interpreting plasma BNP levels in heart failure practice. J Cardiol 2021;78(4):269-74. (In eng). DOI: 10.1016/j.jjcc.2021.05.003.
- Maisel AS, Shah KS, Barnard D, et al. How B-type natriuretic peptide (BNP) and body weight changes vary in heart failure with preserved ejection fraction compared with reduced ejection fraction: secondary results of the HABIT (HF Assessment With BNP in the Home) trial. J Card Fail 2016;22(4):283-93. (In eng). DOI: 10.1016/j.cardfail.2015.09.014.
- Horiuchi Y, Villacorta H, Maisel AS. Natriuretic peptide-guided therapy for heart failure. Heart Int 2022;16(2):112-16. (In eng). DOI: 10.17925/HI.2022.16.2.112.
- Fujimoto Y, Maeda D, Kagiyama N, et al. Prognostic implications of six-minute walking distance in patients with heart failure with preserved ejection fraction. Int J Cardiol 2023;379:76-81. (In eng). DOI: 10.1016/j.ijcard.2023.03.025.
- Grundtvig M, Eriksen-Volnes T, Ørn S, et al. Six min walk test is a strong independent predictor of death in outpatients with heart failure. ESC Heart Fail 2020;7(5):2904-11. (In eng). DOI: 10.1002/ehf2.12900.
- Zotter-Tufaro C, Mascherbauer J, Duca F, et al. Prognostic significance and determinants of the six-min walk test in patients with heart failure and preserved ejection fraction. JACC Heart Fail 2015;3(6):459-66. (In eng). DOI: 10.1016/j.jchf.2015.01.010.
- Wolsk E, Kaye D, Borlaug BA, et al. Resting and exercise haemodynamics in relation to six-minute walk test in patients with heart failure and preserved ejection fraction. Eur J Heart Fail 2018;20(4):715-22. (In eng). DOI: 10.1002/ejhf.976.
- Kamiya K, Sato Y, Takahashi T, et al. Multidisciplinary cardiac rehabilitation and long-term prognosis in patients with heart failure. Circ Heart Fail 2020;13(10):e006798. (In eng). DOI: 10.1161/CIRCHEARTFAILURE.119.006798.
- Sachdev V, Sharma K, Keteyian SJ, et al. Supervised exercise training for chronic heart failure with preserved ejection fraction: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation 2023;147(16):e699-e715. (In eng). DOI: 10.1161/CIR.0000000000001122.
- Ekström M, Li PZ, Lewthwaite H, Bourbeau J, Tan WC, Jensen D. The modified Borg/six-min walk distance ratio: a method to assess exertional breathlessness and leg discomfort using the six-min walk test. ERJ Open Res 2023;9(5) (In eng). DOI: 10.1183/23120541.00281-2023.
Article citation: Del Rio-Pertuz G, Leelaviwat N, Devolder M, Argueta E, Nugent K. The correlation between brain natriuretic peptide levels and six-minute walk distances in patients with heart failure with a preserved ejection fraction. The Southwest Journal of Medicine. 2026;14(60):44-49
From: Department of Medicine, University of Minnesota, Minneapolis, MN (GDR-P) Department of Internal Medicine, Texas Tech University Health Sciences Center, Lubbock, Texas (NL, MD, KN) Department of Cardiology, Baylor Scott and White, Fort Worth, Texas (EA)
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.