ABSTRACT
This patient has a complex medical history that includes intellectual disability, blindness, deafness, seizure disorder, tracheomalacia, and recurrent aspiration. He had a percutaneous endoscopic gastrostomy in place for tube feeding. He again presented with acute respiratory distress, hypoxemia, fever, and leukocytosis. Chest computed tomography (CT) revealed bilateral infiltrates and nodular densities. A previous chest CT done 6 years prior to admission revealed multiple micronodules scattered throughout both lung fields. The patient had had a previous lung biopsy 20 years prior to admission which revealed lentil starch material in bronchioles and multifocal foreign body giant cell reactions. The patient was treated with an empiric antibiotic regimen and improved. This case demonstrates the radiographic and histologic changes associated with lentil pneumonia which is an unusual type of aspiration pneumonia.
Keywords: Lentil pneumonia, granulomas, aspiration, nodules
INTRODUCTION
Patients with significant neurologic impairment or esophageal disorders are at increased risk for aspiration. These episodes usually present with an acute respiratory syndrome that includes fever, leukocytosis, and alveolar infiltrates in dependent lung zones.1 Patients with pulmonary nodules and hilar/mediastinal lymphadenopathy often have an occupational lung disease, granulomatous infection, or diffuse metastatic carcinoma.2 This radiographic appearance would be unusual for aspiration pneumonia, but it can develop when the aspirated material cannot be metabolized by macrophages. Lentil aspiration pneumonia can cause a chronic granulomatous disorder in the lungs and is reviewed in this case report.
CASE
A 69-year-old man with a past medical history of intellectual disability due to prematurity at birth leading to blindness and deafness, asthma, tracheomalacia, seizure disorder, and GERD presented to the emergency room with shortness of breath associated with fever and coughing. This patient has a complex medical history, including multiple prior hospitalizations for recurrent aspiration pneumonia, swallowing dysfunction, and a lung mass. He had a percutaneous endoscopic gastrostomy tube placed seven years ago and does not have oral intake. His vital signs included 85% oxygen saturation on room air, tachycardic with a heart rate 120s beats per minute, and a temperature of 99.5°F. Laboratory results included leukocytosis, anemia, and thrombocytopenia. The patient appeared to be in respiratory distress and was started on high flow nasal cannula 20 liters per minute with a FiO2 of 60%. Computed tomography (CT) of the chest showed mixed perihilar and bilateral pulmonary densities (Figure 1). His previous CT chest from six years ago showed multiple tiny micronodules clustered and scattered throughout both lower lung fields that may be sequelae of granulomatous disease (Figure 2). The patient had a wedge resection lung biopsy twenty years ago that showed presence of lentil starch material in the bronchioles and multifocal foreign body giant cell reaction, subpleural calcified hyalinized nodules, and subpleural fibrosis, consistent with lentil aspiration pneumonia (Figures 3 and 4).
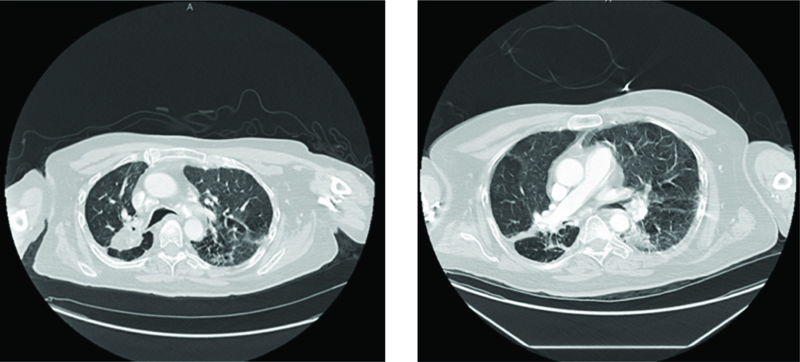
Figures 1A and B. CT chest with contrast showing advanced mixed perihilar and bilateral pulmonary densities with right perihilar bronchial thickening.
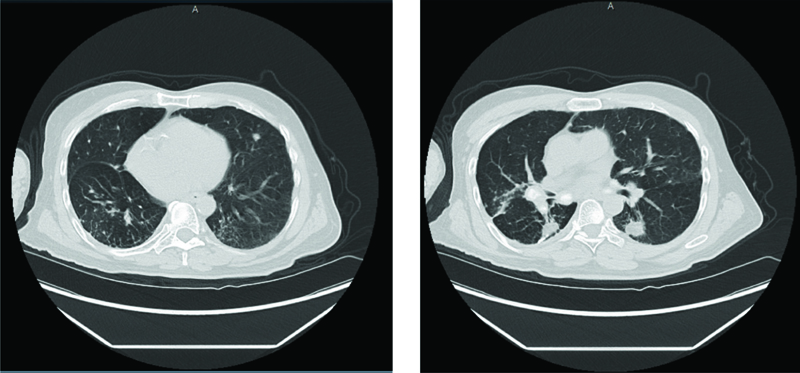
Figures 2A and B. CT chest showed multiple tiny micronodules clustered and scattered throughout both lower lung fields with multiple calcified mediastinal and hilar lymph nodes.
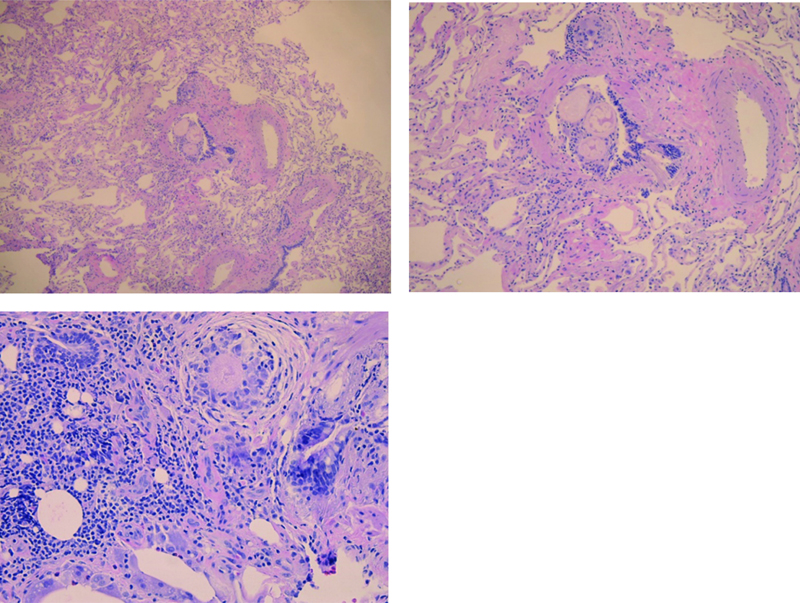
Figure 3. Images (power 5x, 10x & 20x) show lung parenchyma with foreign material (starch; lentil) in the bronchiole with associated foreign body giant cell reaction.
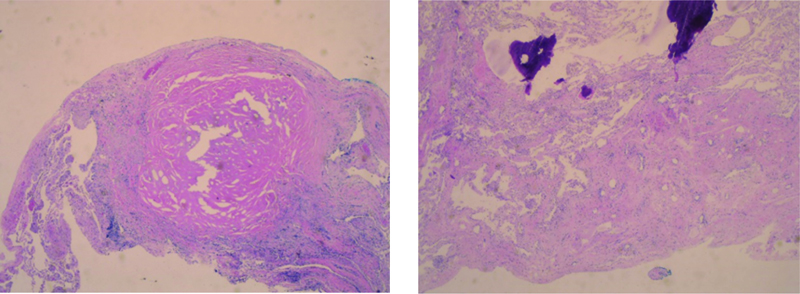
Figure 4. Image on Left: shows hyalinized sclerotic nodule, Image on Right: shows ossification.
DISCUSSION
Lentils are classified as a pulse with other legume seeds, like pea, chickpea, and dry beans.3 Lentil (Lens culinaris spp. culinaris) is a grain legume that is a staple source of dietary protein worldwide. They are a source of bioactive peptides and are rich in protein, dietary fiber, and complex carbohydrates; the seeds are lens shaped. Lentil foods include chickpeas, fava beans, and soybeans. Cultivated lentil proteins are rich in endogenous amino acids (arginine, aspartic and glutamic acids, and leucine-more than half of total amino acids), low in some essential amino acids (threonine, methionine, phenylalanine, tryptophan, histidine, valine, isoleucine, and leucine-excluding lysine), and poor in sulfur-containing amino acids (methionine and cysteine).3
Aspiration of leguminous vegetables, such as lentils, beans, and peas, can cause a non-infectious granulomatous pneumonitis known as lentil aspiration pneumonia that presents on radiologic studies with small, poorly defined nodular opacities.4 Non-infectious granulomatous lung disease is characterized by pulmonary opacities associated with granulomatous inflammation, a relatively nonspecific finding commonly encountered by pathologists. These granulomas have an accumulation of T cells and monocyte macrophages. Patients usually present with pulmonary symptoms or abnormal chest radiographs. Other disorders associated with granulomatous lesions include sarcoidosis, lymphomatous granulomatosis, granulomatous-lymphocytic interstitial lung diseases, talcosis, berylliosis, and hypersensitivity pneumonitis.5
Lentil aspiration pneumonia occurs in medical conditions, such as chronic debilitation, neurologic disorders interfering with swallowing, coughing, and breathing mechanisms, obstetric and emergency surgical procedures, tracheoesophageal fistulas, esophageal stenosis, and achalasia, in which aspiration is common. Predisposing factors in our case included intellectual disability and prior history of aspiration. The aspiration of leguminous vegetable material produces a characteristic histologic pattern of alveolar injury. Initially, it shows acute pneumonitis, often with micro-abscess formation, followed by development of epithelioid granulomas, with or without central necrosis. Demonstration of the aspirated lentil particle, whose durable cellulose content is believed responsible for the granulomatous response, is diagnostic.
Lentil aspiration pneumonia typically has small (1–3 mm) nodular opacities on chest radiographs. Larger nodules (up to 1.0 cm in diameter), as seen in our case, are less common. The opacities are diffuse in distribution, presumably because leguminous vegetables are often cooked as a puree soup and thus aspirated throughout the lungs. The radiologic findings of lentil aspiration pneumonia can be difficult to interpret because they are not typical of aspiration pneumonia, which usually presents as heterogeneous segmental or lobar opacities in dependent portions of lung, and they can be confused with those of other disorders, including hypersensitivity pneumonitis, sarcoidosis, tuberculosis, and metastatic disease. Although the diagnosis should be suspected in patients at risk for aspiration, biopsy and culture are necessary to exclude other diagnoses.6 Most aspiration events involve oral secretions/food or gastric contents. The pathogenesis depends on the acid content, bacterial component (number and virulence), and the presence of particulates. Unusual aspiration-related lung diseases include lipoid pneumonia, foreign body aspiration, and lentils.7 Analyzing the radiographic pattern should expand the differential diagnosis to include less common aspiration syndromes.
REFERENCES
- Neill S, Dean N. Aspiration pneumonia and pneumonitis: a spectrum of infectious/noninfectious diseases affecting the lung. Curr Opin Infect Dis 2019 Apr;32(2):152–157. doi: 10.1097/QCO.0000000000000524.
- Shetty A, Baba Y, Knipe H, et al. Diffuse pulmonary nodules (differential diagnosis). Reference article, Radiopaedia.org. https://doi.org/10.53347/rlD-27258. Accessed 5-23-2024.
- Khazaei H, Subedi M, Nickerson M, et al. Seed protein of lentils: current status, progress, and food applications. Foods 2019 Sep 4;8(9):391. doi: 10.3390/foods8090391.
- Marom EM, McAdams HP, Sporn TA, et al. Lentil aspiration pneumonia: radiographic and CT findings. J Comput Assist Tomogr 1998 Jul–Aug;22(4):598–600. doi: 10.1097/00004728-199807000-00016.
- Franquet T, Franks TJ, Galvin JR, et al. Non-infectious granulomatous lung disease: imaging findings with pathologic correlation. Korean J Radiol 2021 Aug;22(8):1416–1435.
- Marom EM, McAdams H, Sporn T A, et al. Lentil aspiration pneumonia: radiographic and CT Findings. J Computer Assisted Tomography 1998;22(4):598–600.
- Prather AD, Smith TR, Poletto DM, et al. Aspiration-related lung diseases. J Thorac Imaging 2014 Sep;29(5):304–309. RLD–27258. doi: 10.1097/RTI.0000000000000092.
Article citation: Haque T, Basera P, Arif D, Singh T. Lentil aspiration pneumonitis. The Southwest Respiratory and Critical Care Chronicles 2024;12(52):29–32
From: Abrazo Health Internal Medicine (TH), Phoenix, AZ; Icahn School of Medicine Mount Sinai Morningside/West program (PB), New York City, NY; Departments of Pathology (DA) and Internal Medicine (TS), Texas Tech University Health Sciences Center, Lubbock, Texas
Submitted: 4/26/2023
Accepted: 6/20/2024
Conflicts of interest: none
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.